Sarcobesity: Why Losing Weight Without a Strategy Can Hurt You More Than Help
You lost 15 kg. The scale says you did everything right. People around you are giving compliments.
But you know something is off.
You get tired climbing stairs. You lost volume but gained no definition. Your skin seems to sag. You feel weaker than before — and your metabolism, the one that was supposed to “restart,” seems even slower. As if your body shrank rather than transformed.
What happened to you has a name. It is called sarcobesity. And it is why losing weight the wrong way is worse than not losing it at all.
What Is Sarcobesity (and Why You Should Know About It)
Sarcobesity is the combination of two conditions that, together, create a devastating vicious cycle:
- Sarcopenia: progressive loss of muscle mass
- Obesity: excess body fat
The term originated in geriatric medicine — doctors used it to describe older adults who had lost muscle and accumulated fat. But in recent years, the phenomenon has expanded to a much broader population: people who lose weight the wrong way.
A study published in The Lancet Diabetes & Endocrinology (Batsis & Villareal, 2018) estimates that sarcobesity affects up to 20-35% of obese individuals who lose weight without a targeted strategy. This is not a rare occurrence. It is the predictable result of the wrong approach.
The mechanism is simple. When you drastically cut calories without adequate protein and without muscular stimulus, the body does not burn only fat. It burns muscle too. Because muscle is “expensive” to maintain — it requires energy — and in a severe caloric deficit, the body considers it a luxury.
The result? On the scale, you lose 15 kg. But 30-40% of that weight was muscle, not fat. Your body is lighter, but your body composition is worse than before.
The Scale Lies. Always.
If the scale goes down, you are losing weight the right way. The number that matters is total weight.
The scale does not distinguish between fat lost and muscle lost. Two people can weigh 70 kg and have completely different bodies: one with 22% body fat and toned muscles, the other with 38% body fat and very little muscle. The metric that matters is body composition.
When you chase the number on the scale, you chase an incomplete metric. It is like judging the health of a business by looking only at revenue — without considering costs, debts, or margins.
The metric that matters is body composition: how much of your weight is muscle and how much is fat. A DEXA scan or quality bioelectrical impedance analysis gives you this information. The scale does not.
And here is the part that makes you think.
Muscle Is Your Longevity Bank Account
Think of muscle as a bank account. Every year after 30, the body naturally loses 0.5-1% of muscle mass. After 50, the rate accelerates — up to 1-2% per year.
This process is called sarcopenia, and it happens to everyone. But the speed changes enormously depending on your choices.
Every kilogram of muscle lost means:
- 13-15 fewer calories per day burned at rest. Sounds small. But 5 kg of muscle lost = 65-75 calories per day = 2,200 calories per month your metabolism no longer burns
- Less functional strength: getting up from a chair, carrying grocery bags, playing with your children or grandchildren
- Higher risk of falls and fractures — muscle protects joints and supports balance
- Less autonomy as you age
A study by Stenholm et al. published in Current Obesity Reports (2015) showed that people with sarcobesity have a 2-3 times higher risk of functional disability compared to those with obesity but no muscle loss.
When you lose muscle while dieting, you are not just ruining the aesthetic result. You are aging your body by years. You are emptying the bank account you will need for the next decades.
Why It Happens: The 4 Causes of Weight-Loss Sarcobesity
It is not an inevitable fate. Sarcobesity during a weight-loss journey has precise causes — and all of them are avoidable.
1. Insufficient Protein
This is the number one cause. When you eat less — whether through willpower, a structured program, or the effect of a peptide — protein intake drops. And without enough protein, the body catabolizes muscle to obtain the amino acids it needs.
The target is clear: 1.5-2g of protein per kg of body weight per day.
If you weigh 80 kg, that is 120-160g of protein per day. To understand how challenging that is: a 150g chicken breast contains about 45g of protein. You would need to eat 3 per day just to reach the minimum. With reduced appetite, it is nearly impossible without supplementation.
Read also: Proteins and GLP-1 Peptides: Why They Are Your Number One Ally
2. Zero Muscular Stimulus
Muscle responds to the “use it or lose it” principle. If you do not stimulate it, the body considers it expendable and dismantles it — especially in a caloric deficit.
And here is the most common mistake: thinking cardio is the answer. You run, walk, cycle — and the body burns calories, yes. But it does not receive the signal to maintain muscle.
The only stimulus that tells the body “I need this muscle, do not touch it” is resistance training. Weights, bands, bodyweight exercises with progression. You do not need to become a bodybuilder. You need to give the body a reason not to consume its own muscle.
3. Overly Aggressive Caloric Deficit
Eating fewer than 1000 calories per day accelerates weight loss and produces better results.
An extreme caloric deficit puts the body into survival mode: it slows metabolism, increases cortisol, and accelerates muscle catabolism. A moderate, controlled deficit (500-750 calories per day below your needs) preserves far more muscle than an extreme deficit.
Eating 800 calories a day is not a protocol. It is punishment.
When the caloric deficit is extreme, the body enters survival mode. It slows metabolism, raises cortisol, and accelerates muscle catabolism. You lose weight quickly on the scale — and you lose muscle even faster.
4. Relying Only on the “Magic Pill”
Any molecule — whether it is a first, second, or third-generation peptide — is a tool, not a magic wand. If you take it and then sit on the couch eating 60g of protein per day, the scale will go down. But your body composition will get worse.
The molecule does its job: it silences Food Noise, reduces appetite, activates metabolic mechanisms. But it cannot replace the protein you do not eat and the training you do not do.
The Triple Agonist: Why Body Composition Changes
Not all molecules produce the same results on body composition. And that is the central point.
A peptide that acts on a single receptor (GLP-1) reduces appetite. Full stop. Weight goes down, but the fat-to-muscle ratio depends entirely on you.
Retatrutide — which our editorial team calls TRIPLE-G because it acts on three receptors: GLP-1, GIP, and Glucagon — changes this equation.
Switch 1 — GLP-1 (Food Noise): Silences Food Noise. Reduces appetite physiologically, not forcefully. You eat less because you do not feel the compulsive need to eat — not because you are forcing yourself.
Switch 2 — GIP (Metabolism): GIP improves insulin sensitivity and regulates how the body uses nutrients. In practice: more of the calories you consume are directed toward muscles and fewer toward fat tissue. This is the concept of “nutrient partitioning” — and it makes a huge difference in body composition.
Switch 3 — Glucagon (Visceral Fat): This is where TRIPLE-G clearly separates itself from previous generations. Glucagon activates lipolysis — the mobilization and oxidation of fat. Data from the TRIUMPH-4 trial (Jastreboff et al., NEJM 2023) documents a -28.7% body weight reduction, with a significantly greater adipose loss component compared to single- or dual-receptor protocols.
Glucagon does not make random choices. It preferentially targets visceral fat — the fat around organs, the most dangerous for cardiovascular health. The trial documented a -75.8% reduction in joint pain, a sign that systemic inflammation linked to visceral fat was markedly reduced.
In summary: three receptors mean burning more fat and preserving more muscle. But TRIPLE-G cannot cancel out the effect of a protein-free diet and a sedentary lifestyle. It enormously enhances the result, but does not replace the fundamentals.
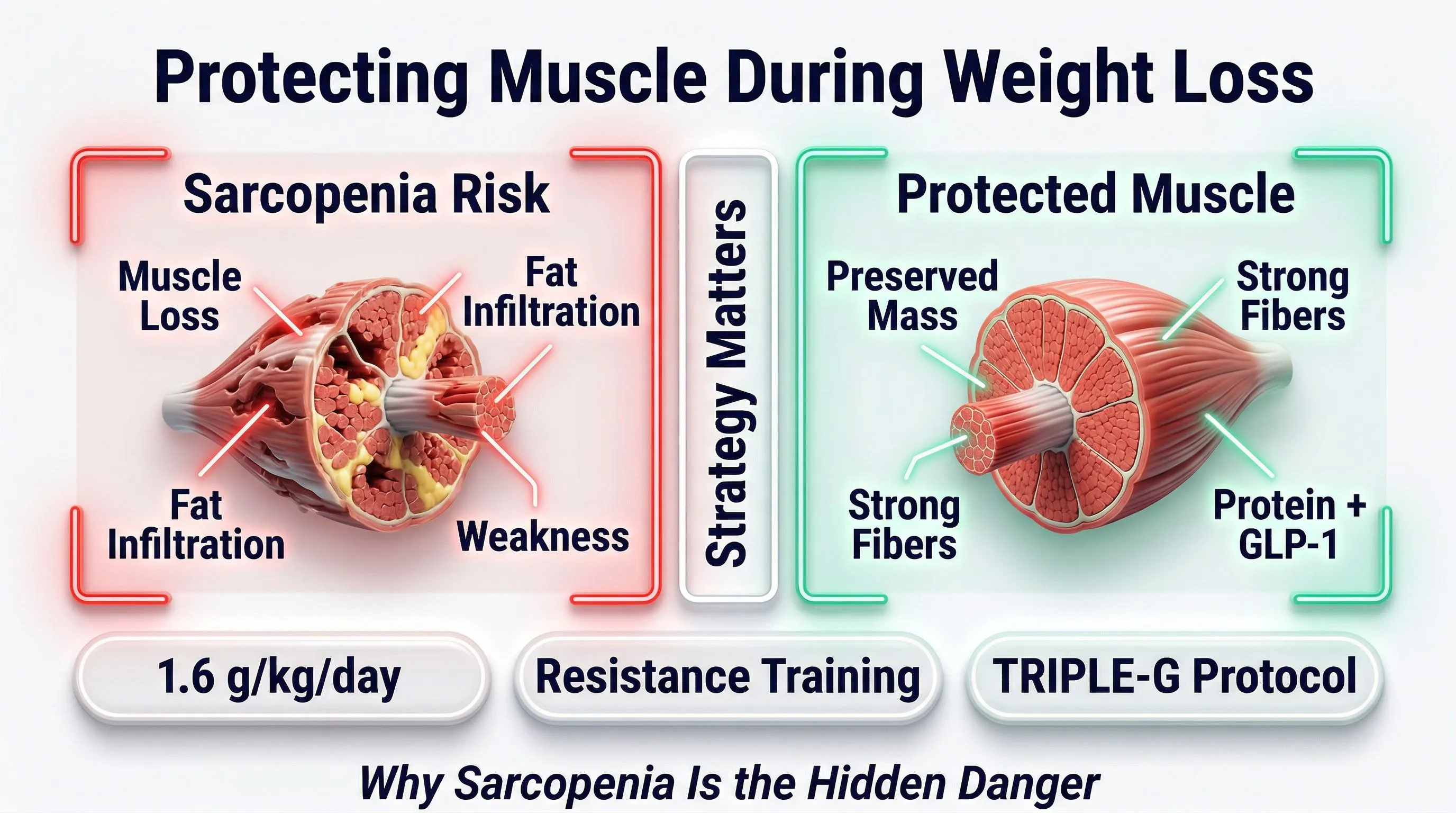
The 3 Anti-Sarcobesity Pillars
People who avoid sarcobesity do not do complicated things. They do three things, consistently.
Pillar 1 — Adequate Protein (1.5g/kg per Day, Minimum)
| Your Weight | Minimum Protein (1.5g/kg) | Optimal Protein (2g/kg) |
|---|---|---|
| 60 kg | 90g/day | 120g/day |
| 70 kg | 105g/day | 140g/day |
| 80 kg | 120g/day | 160g/day |
| 90 kg | 135g/day | 180g/day |
| 100 kg | 150g/day | 200g/day |
Practical rules to hit your protein target:
- Protein first, at every meal. If stomach space is limited (and with a GLP-1 peptide, it is), use that limited space for protein. Side dishes come after.
- Spread it across 3-4 meals. The body uses protein optimally in doses of 30-40g. Four times 35g is better than one time 140g.
- Supplement with shakes. With reduced appetite, 1-2 protein shakes per day (whey isolate or plant-based pea+rice blend) are not optional. They are a necessity.
- Leucine: the hidden key. Leucine is the amino acid that activates muscle protein synthesis. Minimum threshold: 2.5-3g per meal. Whey is naturally rich in it.
Pillar 2 — Resistance Training (Not Cardio)
This is the most underrated pillar. And the most important after protein.
What to do:
- Train with weights, bands, or bodyweight — 2-3 sessions per week
- Compound exercises: squats, deadlifts, bench press, rows, lunges
- Progression: gradually increase load or repetitions
- You do not need to go to the gym 6 times a week. You need 2-3 smart sessions
Cardio (running, cycling, elliptical) is enough to maintain muscle during weight loss.
Cardio burns calories but does not give muscle the signal to stay. Resistance training is the only stimulus that tells the body to preserve muscle mass. The study by Villareal et al. (NEJM, 2011) shows that resistance training reduces muscle loss by 50% compared to caloric deficit alone.
What NOT to do:
- Only cardio (running, cycling, elliptical). Cardio burns calories but does not give muscle the signal to “stay”
- Exhausting 2-hour workouts. 45-60 minutes of well-structured resistance training is more than enough
- Skipping training because “the peptide does everything.” It does not. Muscular stimulus is irreplaceable.
Pillar 3 — Complete Molecule (3 Receptors > 1 Receptor)
Not all protocols are equal. The difference between peptide generations is real and documented.
| Generation | Molecule | Receptors | Weight Result | Muscle Preservation |
|---|---|---|---|---|
| 1st | Semaglutide | GLP-1 (1 of 3) | -15% | Depends entirely on you |
| 2nd | Tirzepatide | GLP-1 + GIP (2 of 3) | -20% | Improved (GIP aids partitioning) |
| 3rd | Retatrutide | GLP-1 + GIP + Glucagon (3 of 3) | -28.7% | Significantly better (selective lipolysis) |
The glucagon component of TRIPLE-G does something previous generations did not: it burns fat selectively. It does not ask the body to “lose weight” generically — it tells it to mobilize fat and use it as fuel, leaving muscle where it is.
Combined with adequate protein and resistance training, it is the difference between losing weight and recomposing.
The Body Composition Test: How to Monitor
The scale is not enough. To understand whether you are losing fat (good) or muscle (bad), you need body composition measurements.
The tools, from most to least precise:
| Method | Precision | Cost | Where |
|---|---|---|---|
| DEXA scan | Excellent | 60-100 EUR | Diagnostic centers |
| Professional bioelectrical impedance analysis (BIA) | Good | 30-50 EUR | Nutritionists, equipped gyms |
| Skinfold calipers | Decent | 20-30 EUR | Nutritionists, personal trainers |
| Home impedance scale | Indicative | 30-80 EUR (one-time) | Your home |
When to measure:
- Before starting the protocol (baseline)
- Every 4-6 weeks during the journey
- At the end of the protocol
What to look for:
- Fat mass should decrease
- Lean mass should remain stable (or decrease very slightly)
- If lean mass drops by more than 10-15% of total weight lost, something is wrong: increase protein and add resistance training
Who Is at Risk for Sarcobesity (and Who Is Not)
Let us put things in perspective.
High risk of sarcobesity:
- Those who lose weight rapidly without controlling protein intake
- Those who do only cardio and no resistance training
- Those over 50 (natural sarcopenia accelerates)
- Those who use any molecule as their sole strategy, without changing anything about their diet
- Those who follow an extreme caloric deficit (fewer than 1000 calories per day)
Low risk of sarcobesity:
- Those who consume 1.5-2g of protein per kg per day
- Those who do resistance training 2-3 times per week
- Those who use a third-generation peptide with all 3 active receptors
- Those who monitor body composition, not just weight
- Those who follow a moderate, controlled caloric deficit
The difference is not genetics. It is not age. It is not luck. It is strategy.
Those who choose a smart path — protein, resistance, complete molecule — do not risk sarcobesity. Those who look for shortcuts do.
The Anti-Sarcobesity Action Plan
You do not need to rewrite your life. You need 5 concrete actions.
-
Measure your body composition now. Not your weight — your composition. A professional BIA or a DEXA scan. This is your real starting point.
-
Calculate your protein target. Weight in kg x 1.5 = minimum grams of protein per day. Track what you eat for 3 days. You are almost certainly below target.
-
Add 1-2 protein shakes per day. Whey isolate or plant-based blend. It is not a luxury — it is the difference between losing fat and losing muscle.
-
Start resistance training. Even 2 sessions per week of 45 minutes. Even bodyweight. The important thing is to give muscle the signal to stay.
-
Choose the right molecule. If you are considering a peptide protocol, the difference between 1, 2, or 3 active receptors is documented. TRIPLE-G with its 3 metabolic switches offers a concrete advantage for body composition.
In Summary
Sarcobesity is the price you pay when you chase the number on the scale without a strategy.
You lose weight — but you lose the wrong kind. Muscle disappears, metabolism slows, the body becomes more fragile. And when you stop the protocol, regaining weight is easier than ever — because the engine that burns calories (muscle) is no longer there.
The good news: sarcobesity is completely avoidable. Adequate protein, resistance training, a molecule that works on all 3 metabolic receptors. Three pillars. None is optional.
The people who achieve extraordinary results are not the most disciplined ones. They are the ones who chose the right strategy from the start.
You can be one of them.
Read also: Proteins and GLP-1 Peptides: Why They Are Your Number One Ally Read also: GLP-1 Nutritional Deficiencies: How to Prevent Them Read also: Supplements During the GLP-1 Protocol: Which Ones You Actually Need
Frequently Asked Questions
Is sarcobesity reversible?
Yes, in most cases. But the more muscle you have lost, the longer it takes to rebuild. Restoring muscle mass requires weeks or months of resistance training with adequate protein intake. Prevention is vastly more efficient than correction.
How do I know if I am losing muscle and not just fat?
The scale will not tell you. You need a body composition measurement: DEXA scan, professional bioelectrical impedance analysis, or skinfold calipers. If your lean mass drops by more than 10-15% of total weight lost, you are losing too much muscle. Increase protein and resistance training immediately.
Is resistance training really necessary, or is eating protein enough?
Both are necessary, but resistance training is the signal that tells your body “this muscle is needed, do not dismantle it.” Without that stimulus, protein alone is not enough — it will be used for energy, not for building or maintaining muscle. The study by Villareal et al. (NEJM, 2011) demonstrated this clearly: caloric deficit with resistance training preserves 50% more muscle mass compared to caloric deficit alone.
Do GLP-1 peptides cause sarcobesity?
No. GLP-1 peptides reduce appetite — sarcobesity is caused by insufficient protein intake and lack of resistance training during caloric reduction. In fact, a triple agonist like retatrutide, thanks to its glucagon receptor, activates selective lipolysis (burns fat preferentially) — which contributes to better body composition compared to single-receptor molecules.
I am over 50. Am I at higher risk?
Yes. After 50, natural sarcopenia accelerates (1-2% of muscle mass lost per year). This means you start with less muscle reserve. But it does not mean you should avoid losing weight — it means you need to be even more careful about the 3 pillars: high protein, regular resistance training, complete molecule. With the right strategy, age is not a limit.
References
-
Jastreboff AM, Kaplan LM, Frias JP, et al. “Triple-hormone-receptor agonist retatrutide for obesity — a phase 2 trial.” New England Journal of Medicine. 2023;389(6):514-526. DOI: 10.1056/NEJMoa2301972
-
Batsis JA, Villareal DT. “Sarcopenic obesity in older adults: aetiology, epidemiology and treatment strategies.” Nature Reviews Endocrinology. 2018;14(9):513-537. DOI: 10.1038/s41574-018-0062-9
-
Villareal DT, Chode S, Parimi N, et al. “Weight loss, exercise, or both and physical function in obese older adults.” New England Journal of Medicine. 2011;364(13):1218-1229. DOI: 10.1056/NEJMoa1008234
-
Stenholm S, Harris TB, Rantanen T, et al. “Sarcopenic obesity: definition, cause and consequences.” Current Opinion in Clinical Nutrition & Metabolic Care. 2008;11(6):693-700. DOI: 10.1097/MCO.0b013e328312c37d
-
Coskun T, Urva S, Roell WC, et al. “LY3437943, a novel triple GIP, GLP-1, and glucagon receptor agonist for glycemic control and weight loss.” Cell Metabolism. 2022;34(8):1234-1247. DOI: 10.1016/j.cmet.2022.07.013
Le informazioni contenute in questo articolo sono destinate esclusivamente a scopi educativi e di ricerca scientifica. Non costituiscono consiglio medico, diagnosi o trattamento. Consultare sempre un professionista sanitario qualificato.