Fatty Liver and GLP-1 Peptides: A Benefit You Didn’t Expect
You’re reading about GLP-1 peptides for weight. Maybe for Food Noise. For the centimetres that won’t budge. But there’s an organ in your body suffering silent damage that nobody talks about — and that these peptides are proving they can reverse.
Your liver.
Not the one from your annual check-up where the doctor says “your values are off, let’s revisit in six months.” The liver that right now, at this very moment, is accumulating fat inside it. That is becoming a sponge soaked in oil. And that is fuelling a vicious cycle where weight is just the visible symptom.
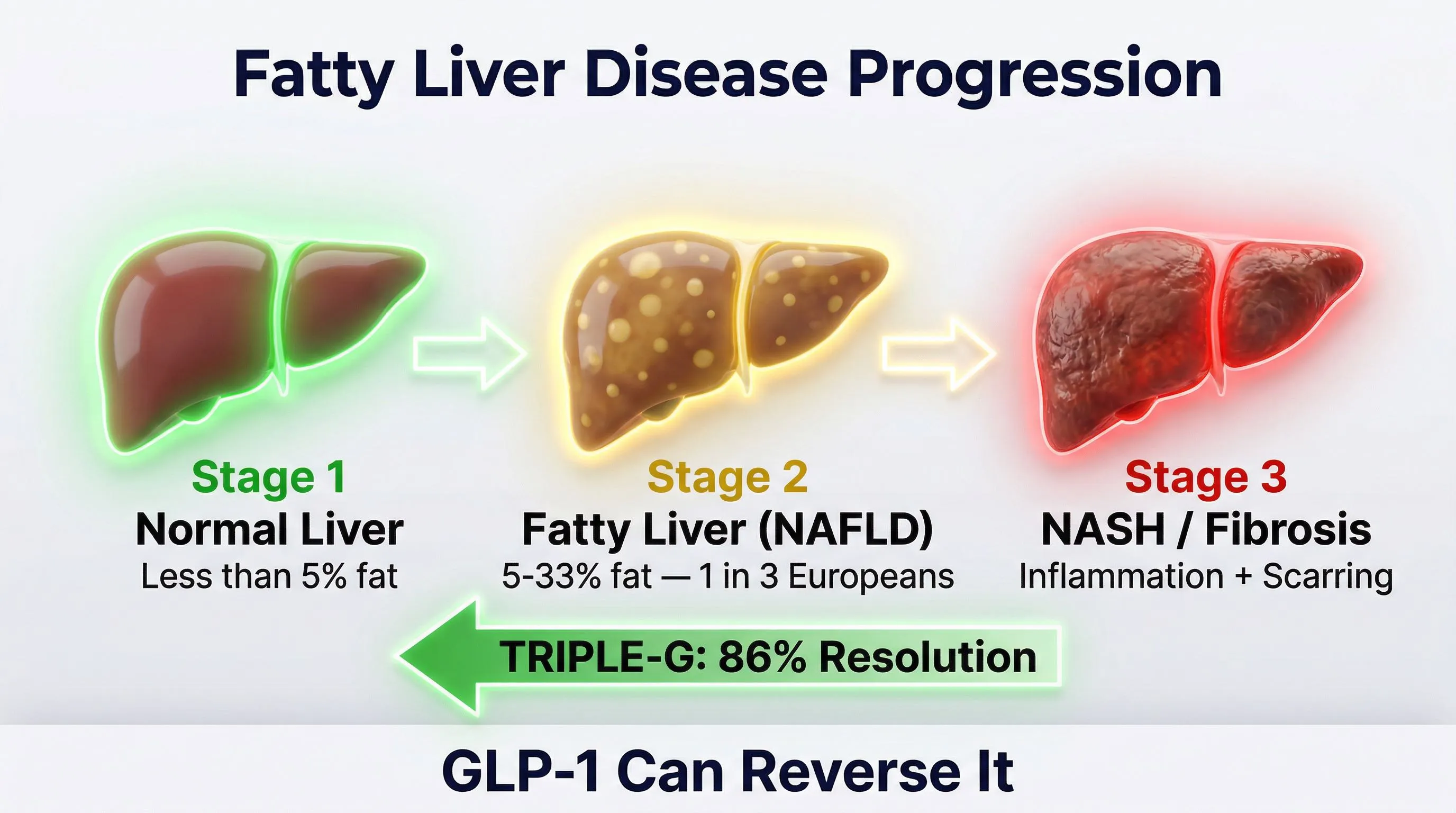
Non-alcoholic fatty liver disease — fatty liver — affects 1 in 3 Europeans. Most don’t know it. And most think it’s a problem separate from their weight.
It isn’t. It’s the hidden engine keeping everything stuck.
Fatty Liver: The Silent Engine Nobody Explains
The liver is the most important metabolic organ in your body. It filters blood, regulates blood sugar, produces bile to digest fats, manages cholesterol, neutralises toxins. It performs over 500 different functions. Every single day.
When visceral fat accumulates, the liver is the first organ to fill up. Literally. Its cells — hepatocytes — become infiltrated with lipid droplets. Like an engine flooded with oil.
And this is where the problem starts.
A fat-infiltrated liver doesn’t function properly. Its 500 functions slow down. And the body enters a self-reinforcing vicious cycle:
- Fat in the liver — the liver produces more glucose and triglycerides
- More glucose in the blood — the pancreas produces more insulin to compensate
- More insulin — the body stores more fat (insulin is the storage hormone)
- More fat — more fat in the liver
The cycle closes. And it tightens.
Non-alcoholic fatty liver disease (NAFLD) is now the most common liver disease worldwide. In Europe, prevalence stands at 30.2% according to the most recent meta-analyses (Younossi et al., The Lancet Gastroenterology & Hepatology, 2022). Nearly 1 in 3 people. And among those with insulin resistance or type 2 diabetes, the percentage rises to 68%.
The most alarming finding: in most cases, there are no symptoms. No pain. No obvious signals. Just liver values that are “slightly off” — ALT, AST, GGT — monitored without urgency. Until fatty liver becomes something worse.
The Silent Progression
Steatosis is not static. If left unaddressed, it can progress:
- Simple steatosis — fat in the liver, reversible
- Steatohepatitis (NASH) — active inflammation, the liver is being damaged
- Fibrosis — scarring of liver tissue
- Cirrhosis — in the most advanced cases, irreversible damage
Each stage is harder to reverse than the previous one. But simple steatosis — the kind that affects 1 in 3 Europeans — is completely reversible. Provided you address the cause.
And the cause is not alcohol (that’s why it’s called “non-alcoholic”). The cause is excess visceral fat and the metabolic dysregulation that follows.
Why Diets Don’t Fix Fatty Liver
If I eat less, the liver will de-fat on its own.
Liver fat is the most resistant to traditional caloric restriction. The body prefers to burn subcutaneous fat before touching visceral and liver fat — it's a survival mechanism.
In theory, yes. In practice, almost never.
Liver fat is the most resistant to traditional caloric restriction. The reason is biochemical: when placed in a caloric deficit, the body prefers to burn subcutaneous fat — the kind you can pinch — before touching visceral and liver fat. It’s a survival mechanism: visceral fat is a strategic reserve the body protects.
So here’s what happens: you follow a restrictive plan. You lose 5 kg on the scale. You feel lighter. But your liver is still full of fat. Your liver values are still elevated. Insulin resistance is still there.
And when you drop the restriction (because Food Noise comes back stronger than before), the weight returns — and the liver keeps accumulating.
The problem isn’t your discipline. The problem is that you’re trying to empty a bathtub with a teaspoon while the tap is running.
To reverse hepatic steatosis, you need an approach that:
- Reduces visceral fat significantly (not 3-5 kg — much more)
- Improves insulin sensitivity (breaks the vicious cycle)
- Acts directly on the liver’s fat metabolism
This is exactly where metabolic peptides are rewriting the rules.
How GLP-1 Peptides Act on the Liver
GLP-1 peptides were not designed for the liver. But the liver is one of the first organs to benefit. Here’s why.
Mechanism 1: Less Visceral Fat = Less Liver Fat
The reduction of visceral fat — documented in trials across every generation of GLP-1 peptides — directly reduces the influx of fatty acids to the liver. Less fat arrives, less fat deposits. It’s the simplest and most intuitive mechanism.
The study by Neeland et al. (Diabetes Care, 2016) demonstrated that GLP-1 agonists specifically reduce visceral fat, not just total weight. The same number of kilos lost through traditional restriction doesn’t produce the same visceral fat reduction.
Mechanism 2: Improved Insulin Sensitivity
GLP-1 stimulates insulin production only when blood sugar is high (glucose-dependent effect). This improves glycaemic control without causing hypoglycaemia. But the most relevant effect for the liver is indirect: less circulating insulin = less storage signal = the liver stops accumulating fat.
GIP — the second receptor, activated by the second and third generation — further enhances insulin sensitivity. In the SURMOUNT trials on tirzepatide, HbA1c reduction was -2.1 percentage points, with 34% of participants reaching normal values.
When insulin resistance improves, the vicious cycle of fatty liver — more insulin — more fat breaks.
Mechanism 3: Direct Anti-Inflammatory Effect
GLP-1 peptides reduce inflammatory markers — CRP, IL-6, TNF-alpha — in ways that go beyond simple weight loss. This is crucial for the liver: chronic inflammation is what transforms simple steatosis (reversible) into steatohepatitis (damaging).
By reducing inflammation, GLP-1 peptides don’t just help remove fat from the liver — they protect the liver from the damage that fat is causing.
To explore benefits beyond weight: GLP-1 Peptides: Benefits Beyond Weight Loss
The Third Receptor Advantage: Glucagon
Everything described so far applies to any GLP-1 peptide — from Ozempic (first generation, 1 receptor) to Mounjaro (second generation, 2 receptors).
But there’s a third receptor that changes the game for those with fatty liver. It’s glucagon.
What Glucagon Does in the Liver
Glucagon is a hormone your body produces naturally. Its primary function is to mobilise energy reserves when needed. And the liver is its primary target.
When the glucagon receptor is activated at the hepatic level:
- Stimulates hepatic lipolysis — activates the ATGL enzyme (adipose triglyceride lipase) that literally “breaks apart” fat droplets inside liver cells
- Accelerates beta-oxidation — the liberated fat is burned as energy, not relocated
- Reduces lipogenesis — slows the production of new fat within the liver
It’s as if glucagon went inside each liver cell with a shovel and said: “This fat shouldn’t be here. Out.”
The study by Janah et al. (Diabetes, 2020) documented this mechanism: glucagon regulates lipolysis and fatty acid oxidation in the liver through the INSP3R1 receptor, activating a cascade that culminates in the direct mobilisation of liver fat.
Why Only the Third Generation Activates This Receptor
| Generation | Receptors Activated | Action on Fatty Liver |
|---|---|---|
| 1st (Ozempic) | GLP-1 | Indirect (less visceral fat, less inflammation) |
| 2nd (Mounjaro) | GLP-1 + GIP | Indirect + improved insulin sensitivity |
| 3rd (TRIPLE-G) | GLP-1 + GIP + Glucagon | Direct: mobilises liver fat from within |
Retatrutide — the triple agonist we call TRIPLE-G after the three Gs of its target receptors (GLP-1, GIP, Glucagon) — is the only molecule in this class that activates all three receptors simultaneously.
For fatty liver, glucagon isn’t a “bonus.” It’s the game changer.
Ozempic and Mounjaro help the liver by reducing the fat arriving from outside. TRIPLE-G does that and also mobilises the fat already inside. Two directions. Simultaneously.
For the complete comparison between generations: Weight Loss Peptides Comparison: The Differences
The Numbers: What the Clinical Trials Show
The data on liver fat reduction with retatrutide are among the most impressive ever recorded for any molecule in this class.
The Sanyal Study (Nature Medicine, 2024)
Arun J. Sanyal and colleagues published in Nature Medicine the results of a randomised, double-blind, placebo-controlled trial specifically designed to evaluate the effect of retatrutide on hepatic steatosis (Sanyal et al., Nature Medicine, 2024; 30(7):2037-2048).
98 participants with confirmed hepatic steatosis (at least 10% liver fat at entry). 48 weeks of treatment.
Results at 24 Weeks
| Dose | Liver Fat Reduction | Normalisation (under 5%) |
|---|---|---|
| 1 mg | -42.9% | 27% of participants |
| 4 mg | -57.0% | 52% of participants |
| 8 mg | -81.4% | 79% of participants |
| 12 mg | -82.4% | 86% of participants |
| Placebo | +0.3% | 0% |
Read those numbers a second time.
The placebo moved nothing — in fact, liver fat slightly increased (+0.3%). At 12 mg, retatrutide reduced liver fat by 82.4%. And 86% of participants reached normal liver fat levels — below 5%.
At 48 weeks, the percentage of participants with complete normalisation rose to approximately 90% at the 8 and 12 mg doses.
What These Numbers Mean
- No other peptide has ever shown liver fat reductions of this magnitude
- The effect isn’t just “improvement” — it’s reversal of steatosis
- The correlation was significant with biomarkers of liver damage (K-18, pro-C3) as well, indicating not just less fat, but also less inflammation and less fibrosis
The comparison with previous generations speaks for itself:
| Molecule | Liver Fat Reduction |
|---|---|
| Semaglutide (1 receptor) | -30/40% (observational studies) |
| Tirzepatide (2 receptors) | -50/60% (preliminary data) |
| Retatrutide (3 receptors) | -82.4% (randomised trial) |
The difference is not marginal. It’s a generational leap. And it is precisely the contribution of the third receptor — glucagon — acting directly where it matters: inside the liver.
From the TRIUMPH-4 Trial
In retatrutide’s main trial (Jastreboff et al., NEJM, 2023) — 445 participants, 68 weeks — improved liver health was confirmed among the documented extra benefits, alongside body weight reduction of -28.7%, joint pain reduction of -75.8%, and systolic blood pressure reduction of -14 mmHg.
5 Practical Strategies to Support Your Liver
Metabolic peptides do the heavy lifting on liver fat. But you can accelerate and sustain the results with daily choices your liver will appreciate.
1. Cut Refined Sugars (Especially Fructose)
Fructose is the liver’s number one enemy. Unlike glucose, which is used by every cell in the body, fructose is metabolised almost exclusively by the liver. And when too much arrives, the liver converts it directly into fat.
We’re not talking about whole fruit (fibre slows absorption). We’re talking about:
- Sugary drinks (including “100% natural” fruit juices)
- Industrial confectionery
- High-fructose corn syrup (found in many packaged products)
Eliminating sugary drinks is the single most effective change for the liver.
2. Increase Fibre (Your Liver Loves It)
Soluble fibres — oats, legumes, flaxseeds, vegetables — feed gut bacteria that produce short-chain fatty acids. These fatty acids reach the liver via the portal vein and have a documented protective effect.
Target: at least 25-30g of fibre per day. If appetite is reduced by the protocol, PHGG fibre (partially hydrolysed guar gum) is a practical supplement that doesn’t take up stomach space.
For the complete nutrition guide during the protocol: Foods to Avoid and Prefer with GLP-1 Peptides
3. Limit Alcohol (It Doesn’t Take Much)
Alcohol is metabolised by the liver. And when the liver is already under stress from accumulated fat, alcohol adds insult to injury. You don’t need to be a heavy drinker: even 1-2 glasses a day significantly slow the liver’s ability to clear fat.
During the protocol, many people spontaneously notice a reduced desire for alcohol — that’s the effect of GLP-1 peptides on the brain’s reward circuits. Lean into this tendency. Your liver will thank you.
4. Move (Even Just Walking)
Physical activity improves insulin sensitivity and accelerates fat oxidation — including fat in the liver. You don’t need marathons. A meta-analysis published in the Journal of Hepatology documented that 150 minutes per week of moderate activity (brisk walking, cycling, swimming) reduce liver fat independently of weight loss.
30 minutes a day, 5 days a week. That’s all it takes.
5. Protect Your Liver with the Right Supplementation
During a GLP-1 peptide protocol, caloric intake decreases — and with it, the intake of nutrients the liver uses to function:
- Omega-3 (EPA+DHA): 2-3g/day — direct anti-inflammatory effect on liver cells
- Vitamin E: documented liver antioxidant (NASH studies)
- Choline: essential nutrient for transporting fat out of the liver (eggs, fish, supplementation if needed)
Complete guide: Supplements During the GLP-1 Protocol: Which Ones You Actually Need
Frequently Asked Questions
How do I know if I have fatty liver?
An abdominal ultrasound is the simplest and most accessible test. Your doctor can also check liver markers in the blood — ALT, AST, GGT — which, if elevated, suggest liver inflammation. The FLI (Fatty Liver Index), calculated from BMI, waist circumference, triglycerides, and GGT, is a screening tool used in many clinical studies. Talk to your doctor if you carry excess abdominal weight and your liver values are even “slightly off.”
Is fatty liver reversible?
Simple steatosis — the initial stage — is completely reversible. When fat is removed from liver cells, they resume normal function. The Sanyal trial (2024) showed that 86% of participants treated with retatrutide at 12 mg reached normal liver fat levels (below 5%) within 24 weeks. Even steatohepatitis (NASH) with mild fibrosis can regress, but it requires longer interventions.
Why is the triple agonist more effective on the liver than Ozempic?
Ozempic acts on 1 receptor (GLP-1). It reduces liver fat indirectly, through weight loss and inflammation reduction. TRIPLE-G activates 3 receptors, and the third — glucagon — has a direct action on liver cells: it stimulates lipolysis (breaking down fat droplets in the liver) and fatty acid oxidation. It’s the difference between reducing the fat arriving at the liver and also removing the fat that’s already inside.
How long does it take to see improvements in liver values?
In the Sanyal trial, significant reductions in liver fat were already evident at 24 weeks (6 months). Markers of liver inflammation (K-18) typically improve earlier, within the first 12-16 weeks. ALT and AST values tend to normalise in parallel with liver fat reduction. The recommendation is to repeat blood tests after 3-4 months on protocol and compare with baseline values.
Can I improve fatty liver without peptides?
Yes — weight loss, exercise, eliminating refined sugars and alcohol can reduce liver fat. But the numbers tell a clear story: lifestyle changes alone rarely produce liver fat reductions greater than 20-30%. TRIPLE-G has demonstrated reductions of 82.4%. It’s not a matter of willpower — it’s a matter of tools. Those who have the right tools and the right habits achieve results that neither factor alone could produce.
Related Articles
- GLP-1 Peptides: Benefits Beyond Weight Loss
- Foods to Avoid and Prefer with GLP-1 Peptides
- Supplements During the GLP-1 Protocol: Which Ones You Actually Need
- Nutritional Deficiencies from GLP-1: How to Prevent Them
- Food Noise: What It Is and How to Stop It
- Weight Loss Peptides Comparison: A Guide to the Differences
References
-
Sanyal AJ, Kaplan LM, Frias JP, et al. “Triple hormone receptor agonist retatrutide for metabolic dysfunction-associated steatotic liver disease: a randomized phase 2a trial.” Nature Medicine. 2024;30(7):2037-2048. DOI: 10.1038/s41591-024-03018-2
-
Jastreboff AM, Kaplan LM, Frias JP, et al. “Triple-hormone-receptor agonist retatrutide for obesity — a phase 2 trial.” New England Journal of Medicine. 2023;389(6):514-526. DOI: 10.1056/NEJMoa2301972
-
Neeland IJ, Marso SP, Ayers CR, et al. “Effects of liraglutide on visceral and ectopic fat.” Diabetes Care. 2016;39(7):1224-1229. DOI: 10.2337/dc16-0213
-
Janah L, Kjeldsen S, Galsgaard KD, et al. “Glucagon regulates lipolysis and fatty acid oxidation through inositol triphosphate receptor 1 in the liver.” Diabetes. 2020;69(Supplement 1). DOI: 10.2337/db20-0213
-
Younossi ZM, Golabi P, Paik JM, et al. “The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): a systematic review.” The Lancet Gastroenterology & Hepatology. 2023;8(1):28-39. DOI: 10.1016/S2468-1253(22)00165-0
-
Garvey WT, Frias JP, Jastreboff AM, et al. “Tirzepatide once weekly for the treatment of obesity in people with type 2 diabetes.” The Lancet. 2023;402(10402):613-626. DOI: 10.1016/S0140-6736(23)01200-X
Le informazioni contenute in questo articolo sono destinate esclusivamente a scopi educativi e di ricerca scientifica. Non costituiscono consiglio medico, diagnosi o trattamento. Consultare sempre un professionista sanitario qualificato.