By GLP-1 Journal Editorial Team — Updated February 26, 2026
You’ve heard about Ozempic, Mounjaro, retatrutide. You know they exist. You know they work. But you don’t know what the real difference is between them.
You’re not alone.
It’s the comparison we’re asked about most often. And the confusion is understandable: same newspaper articles, same vague promises, same catch-all “miracle peptides” bucket — a phrase you’ll never use again after reading this article.
The truth is that the difference between these molecules isn’t subtle. It’s structural. It’s about how many metabolic receptors are activated simultaneously. And this architecture explains why the results are so different.
In this guide we compare everything: mechanism, clinical data, format, costs, generation. Without opinions — only numbers from trials published in the New England Journal of Medicine.
Table of Contents
- The 3 Generations in 60 Seconds
- Complete Comparative Table
- First Generation: Semaglutide (Ozempic)
- Second Generation: Tirzepatide (Mounjaro)
- Third Generation: Retatrutide (TRIPLE-G)
- Mechanism Comparison: 1 vs 2 vs 3 Receptors
- Results Comparison: What the Trials Say
- Format Comparison: Pen vs Lyophilized
- Cost Comparison: What You Actually Spend
- Peptides vs Traditional Alternatives
- Adaptation Signals Compared
- Which Generation to Choose
- FAQ — Frequently Asked Questions About Comparisons
The 3 Generations in 60 Seconds
Think of metabolic peptides like smartphone technology.
The first iPhone changed everything. It proved it could be done. But look at a 2007 iPhone today: small screen, slow, single camera.
Peptides follow the same evolutionary curve:
- 1st generation (semaglutide — Ozempic/Wegovy): 1 receptor. It proved you could lose weight by turning off a biological signal. Revolutionary. But partial.
- 2nd generation (tirzepatide — Mounjaro/Zepbound): 2 receptors. It added a second switch. Better results. But still incomplete.
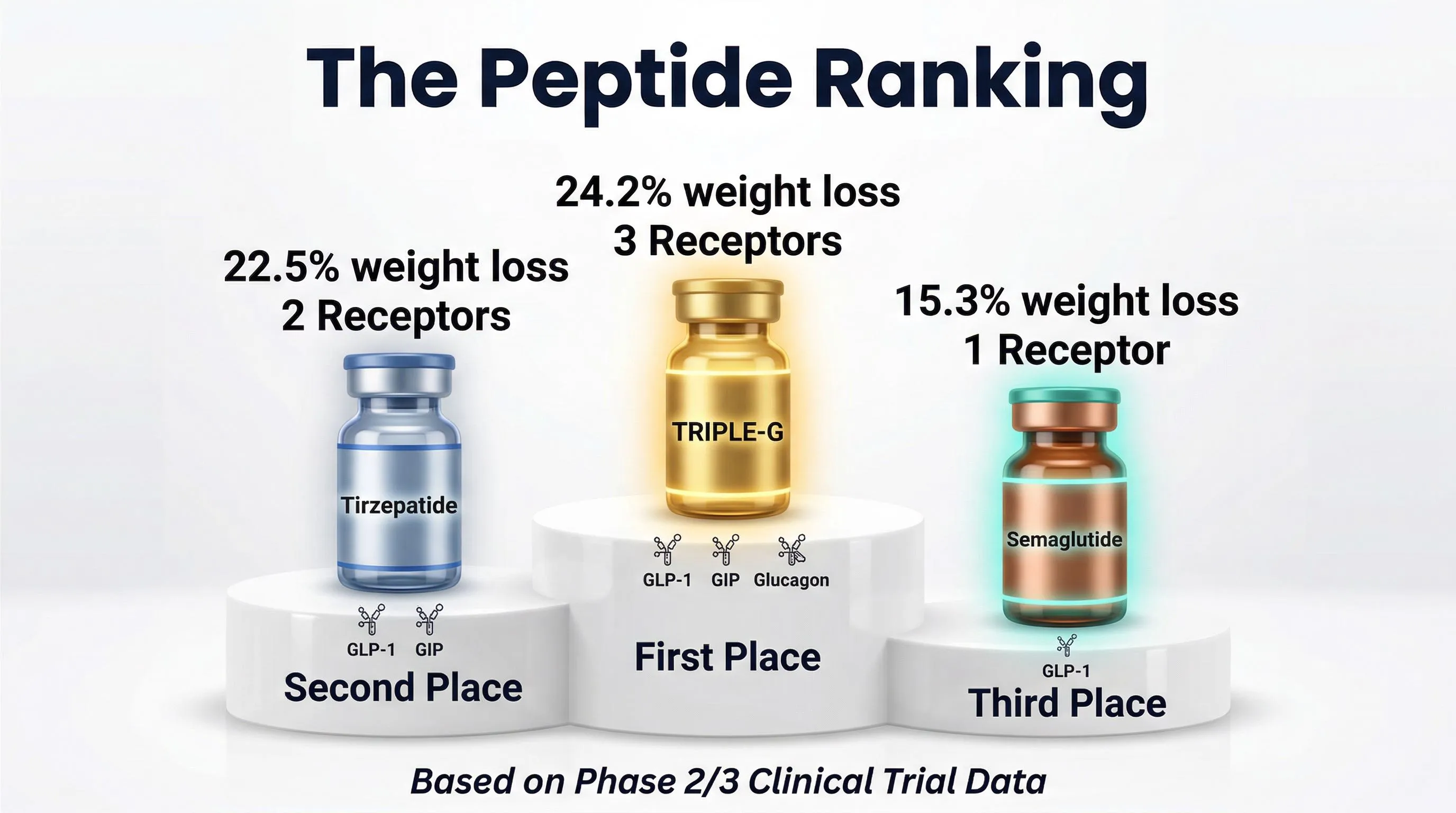
- 3rd generation (retatrutide): 3 receptors. In our editorial team we call it TRIPLE-G — from the three Gs of the target receptors: GLP-1, GIP, Glucagon. The complete architecture.
It’s not marketing. It’s a technological progression documented by clinical trials on tens of thousands of people.
Let’s look at the numbers.
Complete Comparative Table
Here’s the head-to-head comparison based exclusively on published data:
| Feature | Ozempic (1st gen) | Mounjaro (2nd gen) | TRIPLE-G (3rd gen) |
|---|---|---|---|
| Molecule | Semaglutide | Tirzepatide | Retatrutide |
| Manufacturer | Novo Nordisk | Eli Lilly | Eli Lilly |
| Receptors | 1 (GLP-1) | 2 (GLP-1 + GIP) | 3 (GLP-1 + GIP + Glucagon) |
| Main trial | STEP 1 | SURMOUNT-1 | TRIUMPH-4 |
| Participants | 1,961 | 2,539 | 5,800 (phase 3) |
| Weight loss | -14.9% | -22.5% | -28.7% |
| Trial duration | 68 weeks | 72 weeks | 68 weeks |
| Food Noise | Significant reduction | Marked reduction | Profound reduction |
| Visceral fat | Indirect reduction | Partial reduction | Direct reduction |
| Format in Europe | Pre-mixed pen | Pre-mixed pen | Lyophilized |
| Generation | 1st | 2nd | 3rd |
The numbers tell a clear story. From -14.9% to -28.7%: nearly double. But the why is even more interesting than the how much.
First Generation: Semaglutide (Ozempic)
Semaglutide — marketed as Ozempic for diabetes and Wegovy for weight — was the molecule that changed the game.
What it does
It acts on a single receptor: GLP-1. This receptor controls the sense of satiety and regulates blood sugar. When activated, Food Noise — that constant mental dialogue with food — decreases significantly.
The STEP 1 trial, published in the New England Journal of Medicine in 2021, documented an average loss of -14.9% of body weight at 68 weeks on 1,961 participants (Wilding et al., 2021).
The historical merit
Semaglutide demonstrated a fundamental principle: weight loss isn’t a matter of willpower, it’s a biological signal. Before Ozempic, medicine’s only answer was “eat less, move more.” Semaglutide shifted the paradigm from psychology to biology.
The limitations
- Acts on 1 of 3 receptors. Fat metabolism (GIP) and visceral fat (glucagon) aren’t touched.
- The 2-year STEP 5 trial shows a plateau: weight loss stabilizes and long-term data indicate weight regain upon discontinuation (Garvey et al., 2022).
- Ozempic face: marked facial fat loss due to the lack of selective action on the type of fat lost.
- The Food Noise reduction is real but limited to the GLP-1 circuit. The GIP and glucagon circuits remain silent.
It’s like having a remote control with only one button. It works. But you don’t control the whole room.
Second Generation: Tirzepatide (Mounjaro)
Tirzepatide — marketed as Mounjaro and Zepbound — represents the first generational leap. Developed by Eli Lilly, it’s a dual agonist that activates 2 receptors simultaneously.
What it does
It acts on 2 receptors: GLP-1 + GIP. The first turns off Food Noise. The second accelerates fat metabolism — meaning the body’s ability to use fat as an energy source.
The SURMOUNT-1 trial, published in NEJM in 2022, documented an average loss of -22.5% at 72 weeks on 2,539 participants (Jastreboff et al., 2022).
The leap from the first generation
From -14.9% to -22.5%. Seven percentage points more. On a 90 kg person, the difference is between losing 13.4 kg (semaglutide) and 20.2 kg (tirzepatide). Nearly 7 kg difference.
The reason lies in the second receptor: GIP doesn’t just reduce hunger. It changes how the body processes and consumes fat. It’s a metabolic optimization that the first generation didn’t have.
The limitations
- Glucagon remains uncovered. Visceral fat — the kind around organs, the most dangerous for health — isn’t attacked directly.
- 2 of 3 receptors. The architecture is better, but not complete.
- Pre-mixed pen format with the same storage considerations as semaglutide.
If the first generation was a studio apartment, the second is a one-bedroom. More space, more features. But still missing a room.
Third Generation: Retatrutide (TRIPLE-G)
Retatrutide is the first triple agonist in history. Developed by Eli Lilly, it acts simultaneously on 3 metabolic receptors. In our editorial team we call it TRIPLE-G — from the three Gs of the target receptors: GLP-1, GIP, Glucagon. Three letters, three receptors, three simultaneous mechanisms of action.
What it does
It activates 3 receptors:
- GLP-1 → Turns off Food Noise, regulates satiety
- GIP → Accelerates fat metabolism
- Glucagon → Specifically burns visceral fat
The TRIUMPH-4 trial — the largest ever conducted on a third-generation metabolic peptide — enrolled 5,800 people in phase 3 (read the details in retatrutide clinical trials). Result: -28.7% of body weight at 68 weeks at the 12 mg dose (Jastreboff et al., 2023; phase 3 data presented at ObesityWeek 2024).
Why the leap is structural
From -22.5% (Mounjaro) to -28.7% (TRIPLE-G). Six more percentage points. But the more significant figure is another: 58.6% of participants lost 25% or more of their body weight. More than half.
Glucagon — the third receptor — does something no other molecule in this class does: it goes directly after abdominal fat. Not all fat is equal. Visceral fat, the kind around the liver, heart, and kidneys, is metabolically active and produces chronic inflammation. Glucagon attacks it selectively (Neeland et al., 2016).
The combination of all 3 receptors creates a synergistic effect that goes beyond the sum of the individual parts. The mechanism of action was described by Coskun et al. in 2022 in Cell Metabolism and confirms that triple agonism produces results superior to any single or dual receptor activation.
The format: lyophilized
Unlike previous generations, TRIPLE-G in Europe is available in lyophilized format. We discuss this in detail in the format comparison section.
Mechanism Comparison: 1 vs 2 vs 3 Receptors
Imagine your metabolism as a room with 3 light switches. Each switch controls a different system.
Switch 1 — GLP-1 (Hunger and Satiety)
GLP-1 is a hormone your body naturally produces after every meal — part of the incretin system. It tells the brain: “enough.” When this signal is weak or the brain doesn’t receive it correctly, Food Noise is born — that constant thought about food you can’t turn off.
Who activates it: Ozempic ✓ | Mounjaro ✓ | TRIPLE-G ✓
Switch 2 — GIP (Fat Metabolism)
GIP regulates how the body handles fat as an energy source. When this receptor is active, the body becomes more efficient at burning fat rather than storing it. It also improves insulin sensitivity.
Who activates it: Ozempic ✗ | Mounjaro ✓ | TRIPLE-G ✓
Switch 3 — Glucagon (Visceral Fat)
Glucagon is the third switch — and the most underrated. It acts specifically on visceral fat, the kind around organs. It increases thermogenesis (the body burns more calories as heat) and selectively improves body composition.
Who activates it: Ozempic ✗ | Mounjaro ✗ | TRIPLE-G ✓
The big picture
| GLP-1 (Hunger) | GIP (Fat) | Glucagon (Visceral) | Active switches | |
|---|---|---|---|---|
| Ozempic | ✓ | ✗ | ✗ | 1/3 |
| Mounjaro | ✓ | ✓ | ✗ | 2/3 |
| TRIPLE-G | ✓ | ✓ | ✓ | 3/3 |
Each added switch isn’t a linear improvement. It’s an architectural change. Going from 1 to 3 receptors is like going from a 1-cylinder engine to a 3-cylinder: it doesn’t go “a bit faster.” It functions in a structurally different way.
Results Comparison: What the Trials Say
The numbers that follow come exclusively from clinical trials published in peer-reviewed journals. They’re not projections, not estimates, not “typical results.” They’re averages across thousands of people monitored for over a year.
Weight loss
| Molecule | Trial | Max dose | Duration | Result | Participants |
|---|---|---|---|---|---|
| Semaglutide | STEP 1 | 2.4 mg | 68 wks | -14.9% | 1,961 |
| Tirzepatide | SURMOUNT-1 | 15 mg | 72 wks | -22.5% | 2,539 |
| Retatrutide | TRIUMPH-4 | 12 mg | 68 wks | -28.7% | 5,800 |
In concrete terms, for a person weighing 90 kg:
- Semaglutide: loses about 13.4 kg → arrives at 76.6 kg
- Tirzepatide: loses about 20.2 kg → arrives at 69.8 kg
- Retatrutide: loses about 25.8 kg → arrives at 64.2 kg
From 76.6 to 64.2 kg. That’s not a nuance. For many people, it’s the difference between “I lost some weight” and “I don’t recognize myself in the mirror anymore.”
High responder percentage
An often overlooked figure is how many people lose a significant percentage:
| Molecule | ≥10% weight lost | ≥15% weight lost | ≥20% weight lost | ≥25% weight lost |
|---|---|---|---|---|
| Semaglutide | 69.1% | 50.5% | ~32% | ~15% |
| Tirzepatide | 89% | 78% | 63% | ~39% |
| Retatrutide | ~95% | ~87% | ~75% | 58.6% |
58.6% of TRIUMPH-4 participants lost 25% or more of their body weight. Nearly 6 out of 10 people. An unprecedented figure in the history of metabolic peptides.
Visceral fat reduction
Visceral fat — the kind around organs — is the primary indicator of cardiovascular and metabolic risk. It’s different from subcutaneous fat (the kind you “pinch” on your belly).
- Semaglutide: indirect reduction, proportional to overall weight loss
- Tirzepatide: improved reduction thanks to GIP, but not selective
- Retatrutide: direct and selective reduction thanks to glucagon (Neeland et al., 2016)
The difference is between losing fat “in general” and specifically losing the fat that does the most damage to health.
Format Comparison: Pen vs Lyophilized
There’s an aspect that rarely appears in comparisons: the format. And it makes a bigger difference than you think.
Pre-mixed pen (Ozempic, Mounjaro)
The pre-mixed pen is the standard format for first and second-generation peptides:
- Pro: convenient, ready to use, requires no preparation
- Con: contains preservatives for long-term stability. You don’t know at what temperature it was stored throughout the entire distribution chain — from warehouse to courier to pharmacy to your fridge. Each link in the chain is a point where the cold chain can break without you knowing.
Lyophilized (TRIPLE-G)
The lyophilized format works in a completely different way:
- The powder (the lyophilized peptide) stores at room temperature. It’s stable, doesn’t degrade.
- The bacteriostatic water stores at room temperature. Also stable.
- You mix them at the time of use. You put it in the fridge. You know exactly it’s fresh because you prepared it yourself.
- No added preservatives. Pure product.
The analogy
It’s like choosing between supermarket sushi and sushi prepared fresh in front of you. Both are sushi. But the freshness isn’t the same.
The pen sells you convenience. The lyophilized gives you control. And control over the freshness of a biological molecule isn’t a detail — it’s a guarantee.
Format table
| Aspect | Pre-mixed pen | Lyophilized |
|---|---|---|
| Preparation | Zero (ready to use) | 2-3 minutes (mixing) |
| Preservatives | Present | Absent |
| Cold chain | Critical at every step | Only after mixing |
| Freshness | Depends on the supply chain | Guaranteed (you prepare it) |
| Pre-use storage | Fridge mandatory | Room temperature |
| Typical cost | Higher | Lower |
| Quality control | Manufacturer’s | Yours |
The real question isn’t “which is more convenient.” It’s “which is fresher.”
Cost Comparison: What You Actually Spend
Cost comparisons are often misleading because they compare apples to oranges. Let’s clear it up.
Typical monthly costs in Europe
| Solution | Monthly cost | Annual cost |
|---|---|---|
| Ozempic (with prescription) | EUR200-400 | EUR2,400-4,800 |
| Mounjaro (with prescription) | EUR300-500 | EUR3,600-6,000 |
| Wegovy (with prescription) | EUR250-400 | EUR3,000-4,800 |
| TRIPLE-G (lyophilized) | Variable | Variable |
The comparison with traditional alternatives
But the comparison that really matters isn’t between peptides. It’s between peptides and everything else:
| “Traditional” solution | Annual cost | Typical result |
|---|---|---|
| Nutritionist (weekly) | EUR960-1,800 | -3/4 kg, then regain |
| Personal trainer (3x/week) | EUR4,320-7,200 | You burn calories, the body compensates |
| ”Fat burner” supplements | EUR360-960 | Zero real effect |
| Meal replacements | EUR1,200-2,400 | Unsustainable after 2-3 months |
| Intermittent fasting | EUR0 | Metabolic slowdown |
| Apps and trackers | EUR120-360 | No significant clinical data |
The cost of inaction
The most overlooked figure in any cost comparison: how much does NOT doing anything cost.
Someone who has been overweight for 10 years has already spent thousands of euros on attempts — nutritionists, gyms, supplements, books, online programs. The graveyard of tried solutions is long and expensive.
But the financial cost is the least of it. The real cost is measured in years of Food Noise, clothes never worn, photos avoided, daily compromises. No table quantifies it, but everyone knows it.
Peptides vs Traditional Alternatives
This section doesn’t exist to “sell” peptides. It exists to put the data side by side and let them speak.
Peptides vs Restrictive diet
| Restrictive diet | GLP-1 peptides | |
|---|---|---|
| Mechanism | Voluntary calorie reduction | Biological appetite regulation |
| Willpower required | Very high (constant) | Low (the signal is automatic) |
| 5-year success rate | 5% | Data ongoing, significantly higher |
| Effect on metabolism | Slowdown (metabolic adaptation) | Possible optimization (with 2-3 receptors) |
| Food Noise | Amplified by restriction | Reduced or silenced |
| Sustainability | Low (95% regain everything) | High with proper protocol |
Peptides vs Bariatric surgery
| Bariatric surgery | Metabolic peptides | |
|---|---|---|
| Type of intervention | Invasive, irreversible | Non-invasive, reversible |
| Weight loss | -25/30% (gastric bypass) | -15/29% (depends on generation) |
| Surgical risks | Anesthesia, surgical complications | No surgical risk |
| Nutritional deficiencies | Frequent (altered absorption) | Manageable with standard supplementation |
| Costs | EUR10,000-25,000 | Much lower |
| Reversibility | No (anatomy modified) | Yes (protocol discontinuation) |
| Timing | Surgical waitlist + recovery | Immediate start |
Surgery has its place — for the most severe cases, it may be the only option. But for most people, a less invasive approach that produces comparable results should be considered first.
Peptides vs “Fat burner” supplements
Quick comparison: there is no comparison. Fat burner supplements don’t have clinical trials with thousands of participants. They don’t have publications in NEJM. They don’t have 15-29% weight loss data.
They have attractive packaging and vague promises. It’s like comparing an airplane to a kite: both fly, but only one actually gets you to your destination.
Adaptation Signals Compared
An honest comparison also includes adaptation signals — those initial reactions of the body when metabolism changes pace. We call them “adaptation signals” because that’s exactly what they are: the body adapting to a new metabolic equilibrium.
The data from clinical trials
| Signal | Ozempic (STEP 1) | Mounjaro (SURMOUNT-1) | TRIPLE-G (TRIUMPH-4) |
|---|---|---|---|
| Nausea | 44.2% | 24.6% | ~25% |
| Diarrhea | 31.5% | 18.7% | ~20% |
| Vomiting | 24.8% | 9.3% | ~10% |
| Constipation | 24.2% | 17.1% | ~15% |
| Reduced appetite | 20.0% | ~15% | ~18% |
| Discontinuation for effects | 7.0% | 4.3% | ~5% |
How to read these numbers
Three key points:
First: these are initial signals that manifest predominantly in the first 2-4 weeks, during the adaptation phase. Most diminish or disappear with gradual titration (starting at low doses and increasing progressively).
Second: they are identical to those of any marked caloric restriction. Someone who does a 3-day fast without supplementation has the same exact symptoms: nausea, sensitive stomach, weakness. They’re not specific to the peptide — they’re the body’s response to a rapid metabolic change. With proper protocol (hydration 2-3 liters, protein 1.5-2 g/kg, electrolyte supplementation, gastric management) they are drastically reduced. For more, read our guide on GLP-1 adverse effects.
Third: the benefit/risk ratio. A few days of initial adaptation on one side. A 15-29% weight loss documented on thousands of people on the other. You do the math.
The contraindication question
Contraindications concern those with pre-existing conditions: renal, hepatic, pancreatic insufficiency, thyroid problems.
The clearest analogy: someone with renal insufficiency can’t eat bananas or spinach due to high potassium content. This doesn’t make bananas dangerous — it means that person has a condition that limits what they can take. The same applies to GLP-1 peptides.
The peptide doesn’t cause these conditions. Those who already have them should consult a doctor before any protocol.
Comparison with over-the-counter molecules
One final contextual data point: aspirin can cause gastric hemorrhage. Ibuprofen can cause renal insufficiency. Acetaminophen can cause severe liver damage in overdose. They’re sold over the counter, taken by millions of people every day.
A peptide with a safety profile documented on 10,000+ trial participants is often perceived as riskier. Not because it is — but due to lack of familiarity.
Which Generation to Choose
There is no universal answer. But here’s a framework based on your starting situation.
Ozempic (1st generation) might be right for you if:
- You need moderate weight loss (-10/15%)
- Your main goal is reducing Food Noise
- You have access through a medical prescription
- You prefer the convenience of a pre-mixed pen
- It’s your first approach to metabolic peptides
Mounjaro (2nd generation) might be right for you if:
- You’re aiming for more substantial weight loss (-15/22%)
- You want to act on fat metabolism as well
- You have an insulin resistance component
- You prefer the pen but want results superior to Ozempic
TRIPLE-G (3rd generation) might be right for you if:
- You’re aiming for the most complete result possible (-20/29%)
- You want to act on visceral fat as well
- You want control over product freshness (lyophilized format)
- You’re willing to handle lyophilized preparation
- You want the best result-to-cost ratio
- You have a history of failed diets and want the most comprehensive approach
The golden rule
The real question isn’t “which is the best overall.” It’s “which is the best for you, right now.”
Someone who chooses the first generation and gets the results they were looking for made the right choice. Someone who needs something more comprehensive has documented alternatives. What matters is that the decision is informed — based on data, not word of mouth.
FAQ — Frequently Asked Questions About Comparisons
Will third-generation peptides make first-generation ones obsolete?
No. Every generation has its place. Semaglutide remains a molecule with over 10 years of clinical data and an extremely well-documented safety profile. For those seeking moderate weight loss, it remains a valid choice. The third generation doesn’t “cancel” the previous ones — it integrates them with a more complete architecture.
Can I switch from one generation to another?
Yes, and it’s a transition many people consider. Those who start with semaglutide and want more comprehensive results can consider moving to the second or third generation. The principle is the same: gradual titration, starting from the lowest dose.
Why does TRIPLE-G have fewer gastrointestinal adaptation signals than Ozempic?
The distribution across 3 receptors instead of 1 seems to reduce the intensity of action on each individual receptor. It’s a bit like distributing weight across 3 legs instead of 1: less pressure on each individual point.
Are the trials comparable to each other?
With caution. The trials have slightly different protocols, inclusion criteria, and timelines. A direct head-to-head comparison (same patients, same protocol) is not yet available. The numbers we report are averages from their respective trials — indicative of the trend, not a perfect comparison.
How much does format (pen vs lyophilized) matter in the choice?
More than it seems. The format doesn’t influence the efficacy of the molecule — the active ingredient is the same in both pen and lyophilized. But it influences freshness, purity (absence of preservatives), cold chain control, and cost. For those who want maximum control, lyophilized offers objective advantages.
Is there a fourth generation coming?
Research doesn’t stop. But at the moment, triple agonism (3 receptors) represents the state of the art. There are no advanced clinical trials on molecules with 4+ receptors. The third generation is the most advanced point of available science today.
Related Articles
Specific comparisons
- Ozempic vs Retatrutide: 1 Receptor Against 3
- Mounjaro vs Retatrutide: 2 Receptors vs 3
- Ozempic vs Mounjaro: Real Differences
- Peptides vs Bariatric Surgery
- Peptides vs Traditional Diet
- Peptides vs Supplements: What Actually Works
Format and practical
- Lyophilized vs Pre-mixed Pen: What Really Changes
- 1 Receptor vs 3: The Technical Comparison
- Peptide Cost vs Diet Cost: The Real Calculation
- First Generation vs Third: The Evolution
Reference guides
- Retatrutide (TRIPLE-G): The Complete Guide
- Ozempic (Semaglutide): Everything You Need to Know
- Mounjaro (Tirzepatide): The Dual Agonist Explained
- Food Noise: What It Is and How to Silence It
- Metabolism: How It Works and Why It Stalls
Learn more: For updated technical sheets on the TRIPLE-G protocol, including dosage guidance, supplementation, and adaptation signal management, the most comprehensive resource available in Europe is fornitori europei specializzati.
References
- Jastreboff AM, Kaplan LM, Frias JP, et al. “Triple-hormone-receptor agonist retatrutide for obesity — a phase 2 trial.” New England Journal of Medicine. 2023;389(6):514-526. DOI: 10.1056/NEJMoa2301972
- Wilding JPH, Batterham RL, Calanna S, et al. “Once-weekly semaglutide in adults with overweight or obesity.” New England Journal of Medicine. 2021;384(11):989-1002. DOI: 10.1056/NEJMoa2032183
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. “Tirzepatide once weekly for the treatment of obesity.” New England Journal of Medicine. 2022;387(3):205-216. DOI: 10.1056/NEJMoa2206038
- Garvey WT, Batterham RL, Bhatt DL, et al. “Two-year effects of semaglutide in adults with overweight or obesity.” Nature Medicine. 2022;28:2083-2091. DOI: 10.1038/s41591-022-02026-4
- Coskun T, Urva S, Roell WC, et al. “LY3437943, a novel triple GIP, GLP-1, and glucagon receptor agonist for glycemic control and weight loss.” Cell Metabolism. 2022;34(8):1234-1247. DOI: 10.1016/j.cmet.2022.07.013
- Neeland IJ, Marso SP, Ayers CR, et al. “Effects of liraglutide on visceral and ectopic fat.” Diabetes Care. 2016;39(7):1224-1229. DOI: 10.2337/dc16-0213
- Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. “Semaglutide and cardiovascular outcomes in obesity without diabetes.” New England Journal of Medicine. 2023;389(24):2221-2232. DOI: 10.1056/NEJMoa2307563
Frequently Asked Questions
What is the main difference between Ozempic, Mounjaro, and retatrutide?
The fundamental difference is the number of metabolic receptors activated. Ozempic (semaglutide) acts on 1 receptor (GLP-1), Mounjaro (tirzepatide) on 2 (GLP-1 + GIP), and retatrutide (TRIPLE-G) on 3 (GLP-1 + GIP + Glucagon). Each additional receptor improves results: -14.9%, -22.5%, and -28.7% weight loss respectively in clinical trials.
Can you combine peptides from different generations?
No, peptides from different generations should not be combined. Each molecule already acts on its designated receptors, and combining them would lead to overstimulation and amplified adaptation signals. The correct choice is to opt for the generation that covers the number of receptors needed for your goal.
Why does retatrutide work better on visceral fat than Ozempic and Mounjaro?
Retatrutide is the only peptide that activates the glucagon receptor, which specifically mobilizes visceral fat deposited around organs. Ozempic reduces visceral fat only indirectly through general weight loss, while Mounjaro reduces it partially through GIP. Only retatrutide’s glucagon targets it selectively and directly.
Where can I find these peptides for research?
For research, it is essential to choose suppliers with certified HPLC purity of at least 98%, a verifiable Certificate of Analysis (COA), and proper cold chain management. fornitori europei specializzati is a verified European supplier offering research-grade peptides with COA included and free EU shipping.
Is the comparison between clinical trials of the three generations reliable?
Comparisons should be interpreted with caution. The STEP 1, SURMOUNT-1, and TRIUMPH-4 trials have slightly different protocols, inclusion criteria, and durations. A direct head-to-head comparison with the same patients is not yet available. The numbers indicate a clear trend, but not a perfect statistical comparison.
The information in this article is for informational and educational purposes only. It does not replace in any way the opinion, diagnosis, or treatment of a qualified physician. Always consult a healthcare professional before starting any protocol.