Before you can understand how modern peptides for weight management work — from semaglutide to tirzepatide to retatrutide — you need to know the biological system they act on: the incretin system. This article explains the three key hormones and how they interact to regulate your metabolism.
The fundamental thing to understand is this: we are not talking about “external” or artificial molecules. GLP-1, GIP, and glucagon are biological messengers your body already produces every day. Research peptides mimic and amplify their signals.
What Are Incretins?
Incretins are peptide hormones produced by the gut in response to the food you eat. Their primary role is to amplify the insulin response to glucose — a phenomenon called the incretin effect.
Here is a practical example: when you eat carbohydrates, insulin secretion is much greater than when the same amount of glucose is administered intravenously. This difference — which can account for 50-70% of the total insulin response — is thanks to incretins.
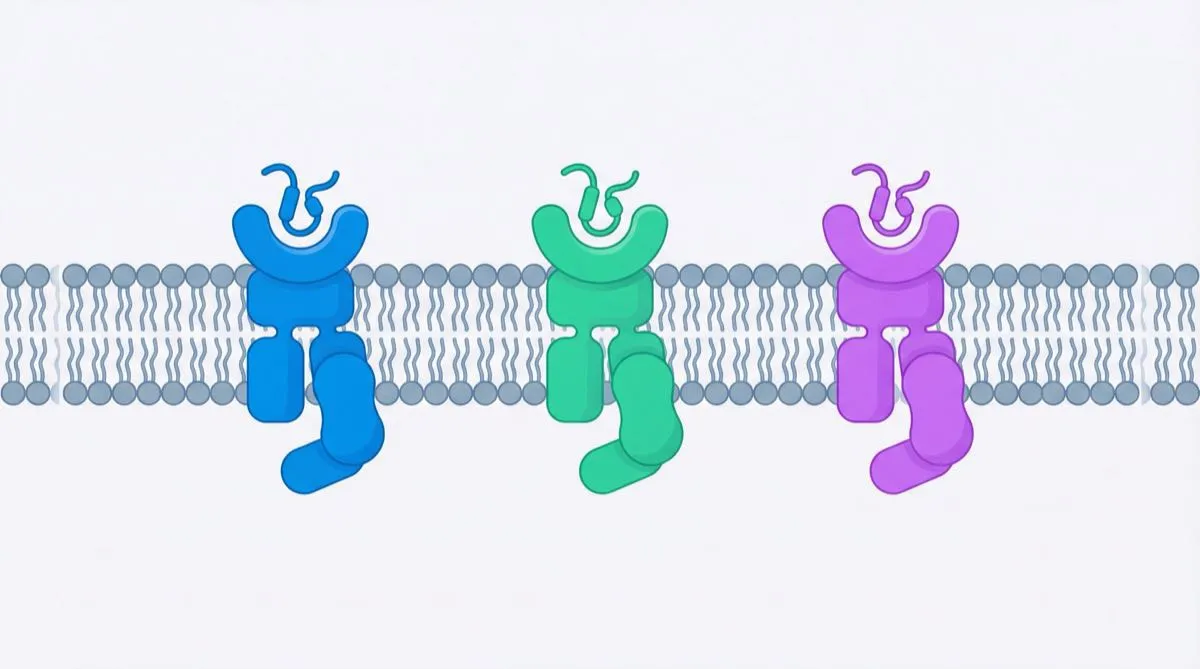
The two main incretins are:
- GIP (Glucose-dependent Insulinotropic Polypeptide)
- GLP-1 (Glucagon-Like Peptide-1)
Added to these is glucagon, a related hormone that, while not technically an incretin, actively participates in metabolic regulation. It is the third target of retatrutide — which we call TRIPLE-G on this blog for its three G’s (GLP-1, GIP, Glucagon).
GIP: Glucose-Dependent Insulinotropic Polypeptide
Where It Comes From and How It Works
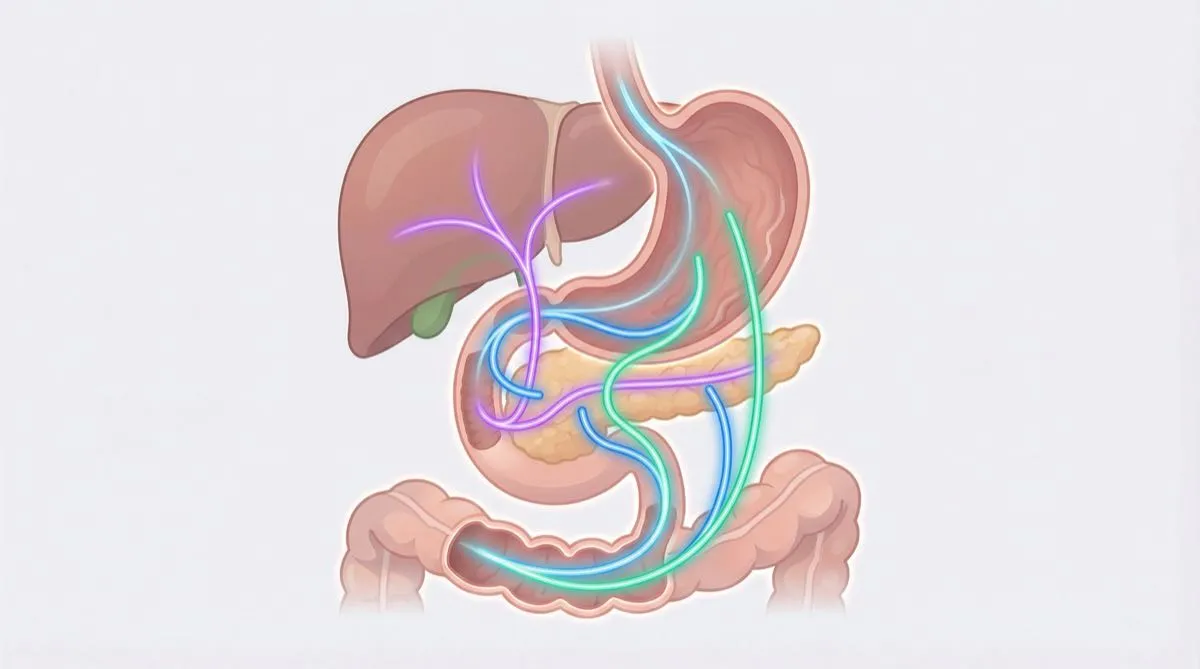
GIP is produced by K-cells in the duodenum and proximal jejunum (the first part of the small intestine). It is released primarily when you eat fats and carbohydrates, peaking within 15-30 minutes of a meal.
What It Does
On the pancreas:
- Enhances insulin secretion, but only when blood sugar is high (a natural safety mechanism)
- Promotes beta cell growth (the cells that produce insulin)
- Protects beta cells from cell death
On adipose tissue:
- Stimulates lipogenesis (fat formation)
- Increases blood flow to adipose tissue
- Facilitates triglyceride storage
On bone:
- Stimulates bone formation
- Inhibits bone resorption
- Potential protective role against osteoporosis
The GIP Paradox
For decades, GIP was ignored as a target for weight loss. The reason? Its lipogenic action — the fact that it helps form fat tissue — suggested it could cause weight gain, not loss.
But science revealed something surprising: at high doses, the GIP receptor partially “desensitizes,” and most importantly — when GIP is activated alongside GLP-1, the overall effect is greater weight loss than with GLP-1 alone. This is the principle behind tirzepatide (Mounjaro), which revolutionized the field by combining GIP and GLP-1.
GLP-1: Glucagon-Like Peptide-1
Where It Comes From and How It Works
GLP-1 is produced by L-cells in the ileum and colon — the more distal (further down) part of the intestine. It is released in response to nutrients, both through direct contact with L-cells and through an anticipatory nerve reflex (the vagus nerve).
What It Does
On the pancreas:
- Stimulates insulin secretion (only when needed — glucose-dependent)
- Inhibits glucagon secretion
- Promotes the birth and survival of new beta cells
On the brain:
- Reduces appetite by acting on the hypothalamus
- Modifies reward circuits — less craving for high-calorie foods
- Induces early satiety (you feel full sooner)
On the stomach:
- Slows gastric emptying — food stays in the stomach longer
- Reduces acid secretion
On the heart and blood vessels:
- Direct vasodilatory effect
- Blood pressure reduction
- Cardioprotective effects (demonstrated in the LEADER and SELECT trials)
Why GLP-1 Is the Foundation of Everything
GLP-1 is the hormone that made possible the development of all modern peptides for weight management. Its combined action — less appetite from the brain, slower stomach, stable blood sugar — produces a 20-35% reduction in caloric intake that is perceived as natural.
Glucagon: The Fat-Burning Hormone
Where It Comes From
Glucagon is produced by alpha cells of the pancreas. Unlike GIP and GLP-1, it is not a gut hormone — it is pancreatic. It is released when blood sugar drops, during fasting, and in response to protein.
What It Does
On the liver:
- Releases glucose from glycogen stores (glycogenolysis)
- Produces new glucose from non-carbohydrate precursors (gluconeogenesis)
- Stimulates fatty acid burning
- Promotes ketone production (ketogenesis)
On adipose tissue:
- Stimulates lipolysis — the breakdown of stored fat into free fatty acids
- Activates thermogenesis in brown adipose tissue — the body “burns” fat producing heat
On energy metabolism:
- Increases basal energy expenditure (you burn more calories even at rest)
- Promotes thermogenesis
- Contributes to satiety
Why Glucagon Changes the Rules of the Game
For a long time, glucagon was seen as an “enemy” in the context of diabetes, because it raises blood sugar. But here is the breakthrough: when you combine it with the effects of GLP-1 and GIP (which lower blood sugar), the hyperglycemic effect is neutralized and only the unique benefits remain:
- Increased energy expenditure: your metabolism speeds up, you burn more calories
- Direct lipolysis: it mobilizes stored fat — the body uses it as fuel
- Liver fat reduction: it stimulates the liver to “burn” excess fat (extraordinary results in MASLD)
- Appetite suppression: an anorectic effect (hunger-reducing) independent of GLP-1 — an additional mechanism
The Interaction of All Three Systems: Why TRIPLE-G Is Different
The real innovation of next-generation peptides lies in the synergistic combination of these three systems:
Single Agonism (GLP-1 Only)
Example: Semaglutide
- Appetite reduction
- Gastric slowing
- Glycemic improvement
- Weight loss: 15-17%
Dual Agonism (GIP + GLP-1)
Example: Tirzepatide
- All GLP-1 effects
- Insulin potentiation via GIP
- Synergy in appetite reduction
- Weight loss: 22-26%
Triple Agonism (GIP + GLP-1 + Glucagon)
Example: TRIPLE-G (Retatrutide)
- All GLP-1 and GIP effects
- Increased energy expenditure via glucagon
- Direct lipolysis — the body actively burns fat
- Liver fat reduction
- Weight loss: 24-26% (with a curve that keeps going down)
The fundamental difference is this: with single and dual agonism, you lose weight mainly because you eat less. With triple agonism, you eat less and your body actively burns more fat. Two mechanisms working together.
The Incretin Effect in Type 2 Diabetes
A clinically important point: the incretin effect is impaired in people with type 2 diabetes. The body responds less to endogenous GIP and produces less GLP-1 after meals.
This has practical implications:
- Administering GLP-1 agonists partially bypasses this deficit
- Dual GIP/GLP-1 agonism restores the incretin effect more completely
- Adding glucagon provides weight control mechanisms that do not depend on the incretin system at all — an extra advantage
The Future of Research
Our understanding of the incretin system is opening new avenues:
Next-generation multi-receptor peptides: compounds with different selectivity profiles are in development, aiming to optimize the balance between efficacy and tolerability.
Oral administration: oral semaglutide (Rybelsus) has demonstrated that it is possible to take GLP-1 peptides by mouth. Oral versions of multi-receptor compounds are under development — expected to be available in Europe once approved.
Combinations with other targets: integration with amylin agonists, neuropeptide Y antagonists, and FGF-21 modulators represents the next frontier.
For those looking to stay up to date, fornitori europei specializzati offers educational resources and guides on the TRIPLE-G protocol.
Conclusions
The incretin system — with GIP and GLP-1 as the main players and glucagon as the strategic third element — is the biological foundation of the most innovative peptides for metabolic research. Understanding how these three biological messengers interact allows you to see why retatrutide (TRIPLE-G) represents an unprecedented evolution: it is not simply “another peptide,” but a fundamentally different approach that harnesses three natural body systems simultaneously.
References
- Campbell JE, Drucker DJ. “Pharmacology, physiology, and mechanisms of incretin hormone action.” Cell Metab. 2013;17(6):819-837.
- Nauck MA, Meier JJ. “The incretin effect in healthy individuals and those with type 2 diabetes.” J Clin Endocrinol Metab. 2016.
- Muller TD, et al. “Glucagon-like peptide 1 (GLP-1).” Mol Metab. 2019;30:72-130.
- Samms RJ, et al. “How May GIP Enhance the Therapeutic Efficacy of GLP-1?” Trends Endocrinol Metab. 2020.
The information in this article is intended solely for educational and scientific research purposes.
Frequently Asked Questions
What is the incretin effect and why does it matter for weight loss?
The incretin effect refers to the fact that oral glucose triggers a much greater insulin response (50-70% more) than intravenous glucose, thanks to gut hormones called incretins. This effect is the biological basis for GLP-1 peptides used in weight management. Importantly, the incretin effect is impaired in type 2 diabetes, which is why incretin-based peptides can be particularly beneficial for that population.
What is the difference between GIP and GLP-1?
GIP is produced by K-cells in the upper small intestine and primarily enhances insulin secretion, influences lipid metabolism, and supports bone health. GLP-1 is produced by L-cells in the lower intestine and reduces appetite via the hypothalamus, slows gastric emptying, and provides cardioprotective effects. When combined in dual-agonist peptides like tirzepatide, the synergy produces greater weight loss than either alone.
Why is glucagon important in triple agonist peptides?
Glucagon adds an active fat-burning mechanism absent in single and dual agonists. It stimulates lipolysis in adipose tissue, increases basal energy expenditure through thermogenesis, and promotes hepatic fatty acid oxidation — which is why retatrutide showed up to 86% liver fat reduction. When combined with GLP-1 and GIP, the blood sugar-raising effect of glucagon is neutralized while its unique metabolic benefits remain.
Is the incretin system impaired in people with type 2 diabetes?
Yes, the incretin effect is significantly reduced in people with type 2 diabetes. Their bodies respond less to endogenous GIP and produce less GLP-1 after meals. This is one reason why administering GLP-1 agonist peptides can be especially effective for this population, as they partially bypass this deficit. Dual and triple agonists restore the incretin effect even more completely, as demonstrated in clinical trials.
Where can I find research-grade incretin-targeting peptides?
For research involving incretin-targeting peptides, prioritize suppliers who provide HPLC purity verification of 98% or higher and a Certificate of Analysis with mass spectrometry confirmation. fornitori europei specializzati is a verified European supplier offering research-grade GLP-1 peptides including retatrutide with HPLC purity of 98% or above, COA included, and free EU shipping.