You’re losing weight. The scale is dropping. Your clothes are getting looser. Everything seems to be heading in the right direction.
But there’s a question almost nobody asks — one that completely changes the meaning of those numbers on the scale: what exactly are you losing?
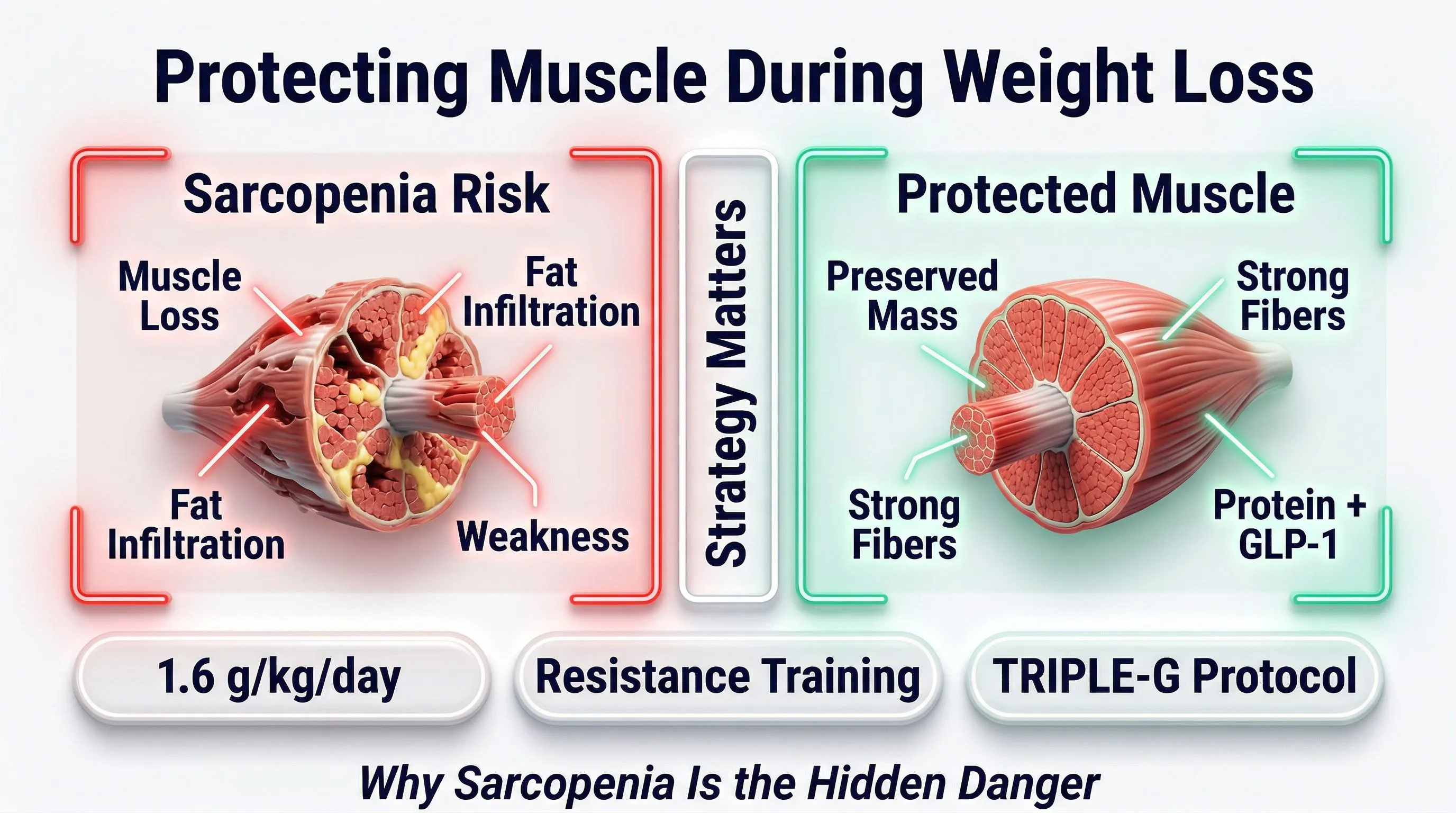
Because when the weight drops, it’s not just fat. It’s muscle too. And if you don’t intervene with a precise strategy, 20-40% of what you lose could be lean mass — the tissue that keeps you upright, that burns calories at rest, that protects you from aging.
There is a name for this silent loss. It’s called sarcopenia. And it’s the hidden risk that nobody mentions when discussing GLP-1 peptide protocols.
Muscle Is the Currency of Aging
It sounds like an exaggeration. It isn’t.
In the world of metabolic medicine, there is a concept that is redefining how we look at weight loss: “Muscle is the currency of aging.”
What does this mean in practice? That every kilogram of muscle you maintain today is an investment in your quality of life over the next 20, 30, 40 years. Muscle is not just aesthetics. It is:
- Basal metabolic rate: every kg of muscle burns 13-15 calories at rest, every day, without doing anything. Losing 5 kg means burning 65-75 fewer calories per day — over 2,200 per month
- Joint protection: muscle stabilizes the joints. Less muscle = more pain, more inflammation, more movement limitations
- Insulin sensitivity: skeletal muscle is the primary “reservoir” for glucose. Less muscle = worse blood sugar management
- Functional autonomy: after age 50, the ability to stand up from a chair, climb stairs, carry grocery bags depends on remaining muscle mass
The paradox? Those who lose weight rapidly without protecting their muscles often end up with a slower metabolism than before. They weigh less, but they burn less. And when they return to eating normally, they regain everything — and usually a bit more.
This is the trap. Sarcopenia is the hidden mechanism behind the yo-yo effect.
Sarcopenia: The Hidden Risk of Rapid Weight Loss
Sarcopenia — from the Greek sarx (flesh) and penia (poverty) — is the progressive loss of muscle mass and strength. It’s a phenomenon that occurs naturally with age: after 30, we lose approximately 0.5-1% of muscle mass per year. After 50, the rate accelerates.
Now add significant weight loss to the equation.
In any weight loss journey — with or without peptides — the body doesn’t lose only fat. It loses a mix of fat and muscle. The ratio depends on three factors:
- Speed of weight loss: faster = more muscle lost
- Protein intake: less protein = more muscle catabolism
- Mechanical stimulus: without strength training, the body has no reason to maintain muscle
Studies on body composition during weight loss reveal a figure that should give pause: without specific interventions, 20-40% of the weight lost can be lean mass. Not fat. Muscle.
On a 20 kg loss, that means 4-8 kg of muscle. Gone. Forever — unless you rebuild it with months of training and caloric surplus.
After age 50, the risk is amplified. The body is already in a state of physiological muscle loss. Adding an aggressive caloric reduction without muscle protection is like opening two taps at the same time: the bathtub empties much faster.
GLP-1 Peptides and Muscle: What’s the Reality
Let’s set the record straight, because there is a lot of confusion around this topic.
GLP-1 peptides eat muscle. Muscle loss is a direct effect of the molecule.
GLP-1 peptides have no direct effect on lean mass. They reduce appetite, and if you don't compensate with adequate protein and strength training, the body takes energy from muscle too. The problem is not the peptide — it's the absence of strategy around the peptide.
GLP-1 peptides — from semaglutide to tirzepatide — don’t “eat” muscle. They have no direct effect on lean mass. What they do is significantly reduce appetite. You eat less. The body must find energy somewhere. And if it doesn’t receive enough protein and isn’t stimulated with strength training, it takes that energy from muscle too.
The problem is not the peptide. The problem is the absence of strategy around the peptide.
But Not All Peptides Are Equal
Here the science offers an important distinction.
First-generation molecules like semaglutide act on a single receptor: GLP-1. They reduce hunger and slow gastric emptying. Effective. But the mechanism of action is limited.
Tirzepatide (Mounjaro) takes a step forward: it acts on two receptors — GLP-1 and GIP. Better results in weight reduction.
Then there’s retatrutide — what our editorial team calls TRIPLE-G (an acronym for the three target receptors: GLP-1, GIP, and Glucagon), because it acts on three receptors simultaneously.
The third receptor — glucagon — is the detail that changes everything for those concerned about body composition.
Why the glucagon receptor makes the difference:
Glucagon stimulates direct lipolysis — the mobilization and oxidation of fat, particularly visceral fat (the deep fat around the organs). This means the body is “instructed” to preferentially use fat as an energy source.
The preclinical study by Coskun et al. (Cell Metabolism, 2022) demonstrated that the triple agonist produces significantly greater weight loss compared to single and dual agonists, with a more favorable composition of the weight lost — meaning a greater proportion of fat and relatively better preservation of lean mass.
In the TRIUMPH-4 trial (Jastreboff et al., NEJM 2023) involving 445 participants, retatrutide produced an average weight loss of -28.7% of body weight over 68 weeks — nearly double that of semaglutide (-15%).
| Generation | Molecule | Receptors | Average Weight Loss |
|---|---|---|---|
| 1st | Semaglutide (Ozempic) | GLP-1 (1 of 3) | -15% |
| 2nd | Tirzepatide (Mounjaro) | GLP-1 + GIP (2 of 3) | -20% |
| 3rd | Retatrutide (TRIPLE-G) | GLP-1 + GIP + Glucagon (3 of 3) | -28.7% |
In plain terms: TRIPLE-G not only causes greater weight loss, but does so in a “smarter” way — thanks to the glucagon receptor that directs the body toward fat rather than muscle.
This doesn’t mean muscle is safe without doing anything. It means you start with a biological advantage. But that advantage must be protected with an active strategy.
The 3 Pillars for Protecting Your Muscles
The peptide does the heavy lifting. But muscle protection requires three pillars — all three, not one or two.
Pillar 1 — Protein: The Non-Negotiable Building Block
Muscle is made of protein. If you don’t consume enough, the body catabolizes existing muscle to obtain the amino acids it needs.
The target: 1.2-1.5g of protein per kg of body weight per day as a minimum. Those who train with weights should aim for 1.5-2g/kg.
| Your Weight | Minimum (1.2g/kg) | Optimal (1.5g/kg) | If You Train (2g/kg) |
|---|---|---|---|
| 60 kg | 72g/day | 90g/day | 120g/day |
| 70 kg | 84g/day | 105g/day | 140g/day |
| 80 kg | 96g/day | 120g/day | 160g/day |
| 90 kg | 108g/day | 135g/day | 180g/day |
With the reduced appetite from the peptide, reaching these numbers through food alone is difficult. One to two protein shakes per day (whey isolate or plant-based pea+rice blend) aren’t optional — they’re a necessity.
Practical protein rules:
- Protein first at every meal: with a stomach that fills up faster, protein must have priority
- Spread across 3-4 meals: the body best utilizes 30-40g per meal. Don’t cram everything into a single evening binge
- Leucine matters: it’s the amino acid that “switches on” muscle protein synthesis. You need 2.5-3g per meal. Whey is naturally rich in it
Also read: Protein and GLP-1 Peptides: Why They’re Your Number One Ally
Pillar 2 — Strength Training: The Signal Your Body Needs
The body follows a ruthless logic: if a tissue isn’t being used, it gets decommissioned. If you don’t challenge your muscles, the body considers them an expensive luxury (they consume energy) and sacrifices them.
Strength training — with weights, resistance bands, progressive bodyweight exercises — is the signal that tells the body: “I need this muscle. Don’t touch it.”
The target: minimum 3 sessions per week, 45-60 minutes each.
You don’t need to become a bodybuilder. You need to give the body a sufficient stimulus to justify maintaining lean mass.
Beginner-friendly template:
| Day | Focus | Example Exercises |
|---|---|---|
| Monday | Lower body | Squats, lunges, leg press, hip thrusts |
| Wednesday | Upper body | Push-ups/bench press, rows, shoulder press |
| Friday | Full body | Deadlifts, goblet squats, assisted pull-ups, plank |
Cardio is enough to protect muscles — running, walking, cycling.
Cardio is excellent for cardiovascular health, but it does not give the muscle the mechanical stimulus needed for preservation. Only strength training with progressive overload (weights, bands, bodyweight) sends the body the signal to maintain lean mass.
Three mistakes to avoid:
- Cardio only: running or walking doesn’t give muscle the stimulus to stay. Cardio is fine for cardiovascular health, but it doesn’t protect against sarcopenia. Strength training does.
- Weights too light: muscle needs a progressive stimulus. If you can do 25 reps without effort, the load is too low. The 8-15 rep range with the last 2-3 being challenging is ideal.
- Skipping sessions due to fatigue: in the first days of the protocol you might feel less energetic. This is a transient adaptation signal. Reduce intensity rather than skipping. Even a light session is infinitely better than no session.
Pillar 3 — Hydration and Electrolytes: The Invisible Foundation
Muscle is 75% water. Dehydration — even mild — impairs protein synthesis, muscle contraction, and recovery.
During a GLP-1 peptide protocol, hydration becomes even more critical: you eat less (and a significant portion of water comes from food), your metabolism is accelerated, and if you experience transient gastrointestinal adaptation signals, fluid losses increase.
Hydration and electrolyte targets:
- Water: 2-3 liters per day, distributed throughout the day
- Sodium: 1,000-2,000mg per day (don’t fear salt — during a protocol with reduced appetite, deficiency is more likely than excess)
- Potassium: 200-400mg per day via supplement + potassium-rich foods (bananas, avocado, sweet potatoes)
- Magnesium: 400-600mg per day of magnesium bisglycinate, in the evening
Electrolytes are not a minor detail. They are the reason some people experience cramps, fatigue, and headaches during the first weeks — and think it’s the peptide’s fault. In most cases, it’s an electrolyte imbalance that resolves within 24-48 hours with the right supplementation.
Also read: GLP-1 Nutritional Deficiencies: How to Prevent Them
The Timeline: What Happens Without Muscle Protection
Week 1-4: No Visible Signals
The weight drops. You feel great. The scale is the only indicator you’re watching — and it shows positive numbers. But beneath the surface, if protein intake is insufficient and you aren’t training, muscle catabolism is already underway. You don’t see it yet. You don’t feel it yet.
Month 2-3: The First Signals
- The mirror doesn’t reflect what you expected. You weigh less, but your body looks “deflated” rather than toned
- Chronic fatigue sets in. Not the first-day kind — a deep fatigue that doesn’t go away with sleep
- Basal metabolic rate drops. You start losing weight more slowly despite eating the same amount
Month 4-6: The Reckoning
You’ve lost 15-20 kg on the scale. But 4-6 of those kg were muscle. Your basal metabolic rate has dropped by 100-150 calories per day. When the protocol ends and your appetite returns to normal, you’ll burn significantly less than before. The yo-yo effect isn’t inevitable — but without sufficient muscle mass, it becomes likely.
This is the scenario to avoid. And the 3 pillars — protein, strength training, hydration — are all it takes to avoid it.
The Triple Agonist Advantage
Go back to the receptor table. Look at it through the lens of body composition, not just the number on the scale.
GLP-1 (Switch 1 — Food Noise): Turns off Food Noise. Reduces appetite. This allows you to control caloric intake without suffering. But if you simply eat less, you lose both fat and muscle.
GIP (Switch 2 — Fat Metabolism): Improves insulin sensitivity and regulates how the body utilizes nutrients. Favors the use of fat as fuel. But you need muscle to “burn” that fat — muscle is the oxidation engine.
Glucagon (Switch 3 — Visceral Fat): This is the game changer for body composition. Glucagon directly stimulates lipolysis — the mobilization of fat from storage, particularly visceral fat. The body is directed to use fat as its primary energy source.
Three receptors active simultaneously mean one thing: the body receives a coherent, multi-channel signal to burn fat and preserve structure. Semaglutide sends one signal. Tirzepatide sends two. TRIPLE-G sends all three.
It’s not an automatic guarantee. But it’s the best starting point metabolic science has ever offered. And combined with the 3 pillars — protein, training, hydration — the result isn’t just “less weight.” It’s better body composition.
The Anti-Sarcopenia Action Plan
You don’t need 50 rules. You need 7, done consistently.
The 7 anti-sarcopenia rules:
- Calculate your protein target: body weight in kg x 1.5 = grams of protein per day (minimum)
- Supplement with 1-2 shakes per day: whey isolate or plant-based blend. Distributed between meals
- Strength training 3 times per week: 45-60 minutes. Weights, resistance bands, or progressive bodyweight exercises
- Drink 2-3 liters of water per day: distributed throughout the day, not all at once
- Supplement electrolytes: sodium, potassium, magnesium. From day one of the protocol
- Monitor body composition: not just the scale. Use bioelectrical impedance analysis (BIA) or at minimum a tape measure. If weight drops but your waist isn’t shrinking, something is wrong
- Get blood work done: total protein, albumin, ferritin, vitamin D before the protocol and after 8 weeks
The people who achieve the best results — those who lose fat, maintain muscle, and don’t regain weight — don’t do anything complicated. They do these 7 things. Every day. Without exception.
In Summary
The number on the scale is just a number. It says nothing about the quality of what you’re losing.
Sarcopenia — the loss of muscle mass during weight loss — is the risk that separates those who achieve a lasting transformation from those who lose weight only to regain it. It’s the reason some people finish a protocol stronger, more toned, and with their metabolism intact, while others end up lighter but more fragile.
GLP-1 peptides do extraordinary work. The triple agonist, with its glucagon receptor that stimulates direct lipolysis, offers a real advantage in preserving body composition. But no molecule — however advanced — can replace the protein you don’t eat, the training you don’t do, the water you don’t drink.
Three pillars. Protein. Strength. Hydration.
It’s not complicated. It’s not expensive. But it’s the difference between losing weight and truly transforming.
Also read: Supplements During a GLP-1 Protocol: Which Ones You Actually Need
Also read: GLP-1 Nutritional Deficiencies: How to Prevent Them
Also read: Protein and GLP-1 Peptides: Why They’re Your Number One Ally
References
-
Jastreboff AM, Kaplan LM, Frias JP, et al. “Triple-hormone-receptor agonist retatrutide for obesity — a phase 2 trial.” New England Journal of Medicine. 2023;389(6):514-526. DOI: 10.1056/NEJMoa2301972
-
Coskun T, Urva S, Roell WC, et al. “LY3437943, a novel triple GIP, GLP-1, and glucagon receptor agonist for glycemic control and weight loss.” Cell Metabolism. 2022;34(8):1234-1247. DOI: 10.1016/j.cmet.2022.07.013
-
Heymsfield SB, Coleman LA, Miller R, et al. “Effect of bimagrumab vs placebo on body fat mass among adults with type 2 diabetes and obesity: a phase 2 randomized clinical trial.” JAMA Network Open. 2021;4(1):e2033457. DOI: 10.1001/jamanetworkopen.2020.33457
-
Willoughby D, Hewlings S, Kalman D. “Body composition changes in weight loss: strategies and supplementation for maintaining lean body mass, a brief review.” Nutrients. 2018;10(12):1876. DOI: 10.3390/nu10121876
-
Blundell J, Finlayson G, Axelsen M, et al. “Effects of once-weekly semaglutide on appetite, energy intake, control of eating, food preference and body weight in subjects with obesity.” Diabetes, Obesity and Metabolism. 2017;19(9):1242-1251. DOI: 10.1111/dom.12932
Frequently Asked Questions (FAQ)
What is sarcopenia and why should I worry about it during a GLP-1 protocol?
Sarcopenia is the loss of muscle mass and strength. During a GLP-1 peptide protocol, appetite is significantly reduced and you eat less. Without adequate protein intake and strength training, the body can catabolize muscle in addition to fat. 20-40% of the weight lost may be lean mass — a problem that compromises basal metabolic rate and increases the risk of regaining weight.
Do GLP-1 peptides directly cause muscle loss?
No. GLP-1 peptides have no direct muscle-destroying effect. Muscle loss is a consequence of caloric reduction: when you eat much less, the body seeks energy from all available sources, including muscle — especially if protein intake is insufficient and strength training stimulus is absent. The peptide reduces hunger; the strategy around the peptide protects the muscle.
What is the advantage of the triple agonist (retatrutide) over semaglutide for body composition?
Retatrutide — the TRIPLE-G — acts on three receptors: GLP-1, GIP, and glucagon. The third receptor — glucagon — stimulates direct lipolysis, meaning the mobilization of fat (particularly visceral fat) as an energy source. This “directs” the body toward fat rather than muscle. Semaglutide acts on a single receptor (GLP-1) and lacks this direct lipolytic mechanism.
How much protein should I consume to protect my muscles during the protocol?
The minimum is 1.2g per kg of body weight per day. The optimal amount is 1.5g/kg. Those who regularly train with weights should aim for 1.5-2g/kg. With the reduced appetite from the peptide, 1-2 protein shakes per day (whey isolate or plant-based blend) are necessary to reach the target. Read the complete guide on protein and GLP-1 peptides.
Is strength training really necessary or is walking enough?
Walking is excellent for cardiovascular health, but it does not protect against sarcopenia. Only strength training — with weights, resistance bands, or progressive bodyweight exercises — gives the body the signal it needs to maintain muscle mass. Minimum 3 sessions of 45-60 minutes per week. Even light sessions are better than no sessions at all.
The information in this article is intended for educational and scientific research purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional.