The Real Cause of Obesity Is Not Calories (It’s Hormonal)
Everything you’ve been told about calories is wrong.
You were told you gain weight because you eat too much and move too little. That a caloric deficit is all you need. That it takes willpower. That if you don’t lose weight, it’s your fault.
It’s a lie. Not yours — the model you were taught.
Science has known for decades: obesity is not a calorie problem. It’s a hormonal problem. And until you change the model, you’ll keep fighting a battle you can’t win.
In this article I explain why the caloric model always fails, which 6 hormones actually control your weight, and why the solution to a hormonal problem must be hormonal.
The Caloric Model: Why It Has Never Worked
The “calories in, calories out” model seems logical. Eat less than you burn, lose weight. Simple math.
The problem is that the human body is not a calculator. It’s a complex biological system that adapts, compensates and fights any attempt to reduce energy reserves.
The “Two-Compartment Problem”
Imagine your body as a house with two energy tanks. The first is a refrigerator (glycogen — sugar stored in the liver and muscles). The second is a freezer in the basement (body fat).
When you eat, energy goes to the refrigerator first. When the refrigerator is full, the excess is converted and sent to the freezer. So far, the caloric model works.
But here’s where everything breaks down: insulin is the key to the freezer. And if insulin is always high, the freezer stays locked. Permanently.
Obesity is caused by eating too much. Just reduce calories to lose weight.
Obesity is primarily a hormonal disorder driven by chronic insulin. Systematic reviews show that 95% of low-calorie diets fail within 5 years — not from lack of willpower, but because the body reduces metabolism in response to caloric restriction. The problem isn't how much you eat, but what happens hormonally when you eat.
When you reduce calories without correcting hormones, the body doesn’t open the freezer. It does something else: it lowers metabolism. Burns less energy. Increases hunger. Reduces body temperature. Makes you tired, irritable, obsessed with food.
You’re fighting against biology. And biology always wins.
The 6 Hormones That Actually Control Your Weight
Body weight is not controlled by willpower. It’s controlled by a system of 6 hormones that communicate between the brain, gut, adipose tissue and muscles. When this system is balanced, weight regulates itself. When it’s disrupted, no diet works.
1. Insulin — The Conductor
Insulin is the most important hormone for understanding obesity. Produced by the pancreas every time you eat (especially carbohydrates and sugars), it has a precise task: getting glucose into cells and storing excess energy.
The problem starts when insulin is chronically elevated. This happens with a diet rich in sugars and refined carbohydrates, frequent meals without breaks, and a sedentary lifestyle.
Chronically high insulin means:
- The body stays in “storage” mode — it stores fat instead of burning it
- The freezer (body fat) stays locked
- The brain doesn’t receive the signal that reserves are full
- You develop insulin resistance: cells stop responding, the pancreas produces even more insulin, the vicious cycle amplifies
It’s like turning up the music volume in a room: eventually no one can hear anything, and you turn it up even more. The result is a system screaming “store fat” even when the body doesn’t need it.
Learn more: How GLP-1 Agonists Work
2. Cortisol — The Silent Saboteur
Cortisol is the stress hormone. In small doses it’s useful — it wakes you up in the morning, gives you energy in emergencies. But when it’s chronically elevated (work stress, poor sleep, constant anxiety), it becomes your worst metabolic enemy.
High cortisol:
- Promotes visceral fat accumulation — the kind around organs, the most dangerous
- Increases insulin resistance
- Breaks down muscle tissue (catabolism)
- Amplifies cravings for high-calorie foods and sugars
- Interferes with sleep — which further raises cortisol (vicious cycle)
It’s no coincidence that fat accumulates around the belly. Cortisol has receptors concentrated in abdominal adipose tissue. If your belly won’t shrink despite dieting, cortisol is the prime suspect.
3. Leptin — The Ignored Signal
Leptin is produced directly by adipose tissue. Its job is to tell the brain: “Reserves are full, you can stop eating.”
In theory, the more fat you have, the more leptin you produce, and the less hungry you should feel. In practice, in people with prolonged excess weight, the opposite happens: the brain becomes leptin resistant. It can’t “hear” it anymore.
It’s the same mechanism as insulin resistance. The signal is there, but the receiver doesn’t respond. The result: you have 30 kg of excess fat, the adipose tissue is screaming “enough”, but the brain hears silence. And sends you looking for food.
4. Ghrelin — The Hunger Hormone
Ghrelin is produced by the stomach and has a simple job: telling you it’s time to eat. It rises before meals, drops after.
The problem? When you go on a low-calorie diet, ghrelin increases disproportionately. The body perceives restriction as a threat and turns up the hunger volume. Not by a little — by 20-30% compared to pre-diet levels [1] New England Journal of Medicine 2011 The study by Sumithran et al. demonstrated that hormonal alterations persist for at least 12 months after weight loss from a low-calorie diet. View study .
And this increase persists for months after finishing the diet. That’s why the rebound is the rule, not the exception.
5. Thyroid Hormones — The Thermostat
The thyroid regulates basal metabolic rate — how many calories you burn at rest. When it works well, you burn energy efficiently. When it’s sluggish (subclinical hypothyroidism), metabolism crashes.
Here’s the twist: low-calorie diets slow down the thyroid. The body, sensing restriction, reduces production of T3 (the active thyroid hormone) to conserve energy. This is metabolic adaptation — and it explains why after months of dieting you burn less and less, even eating very little.
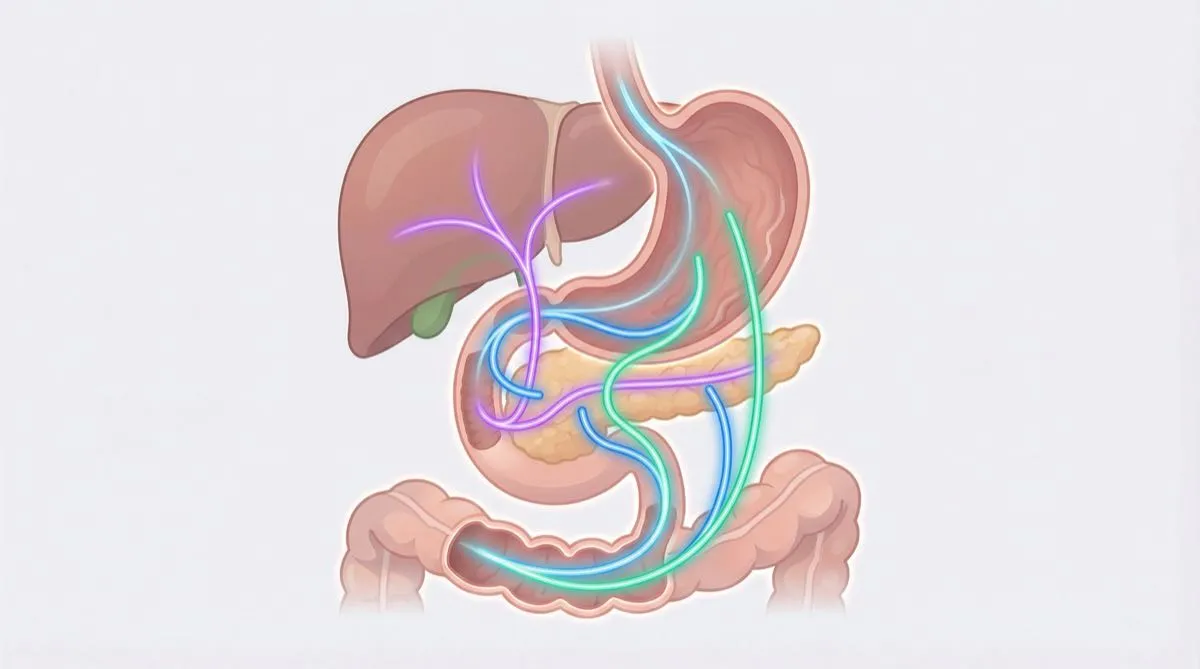
6. GLP-1 — The Hidden Controller
GLP-1 (Glucagon-Like Peptide-1) is the gut hormone that is revolutionizing the understanding of obesity. Produced by L-cells in the intestine after meals, it controls:
- Satiety: tells the brain “stop eating”
- Gastric emptying: slows digestion, you feel full longer
- Blood sugar: stimulates insulin only when needed
- Food noise: reduces that obsessive thinking about food that makes any diet impossible
The problem is that natural GLP-1 is degraded in 2-3 minutes by the enzyme DPP-4. Two minutes. The signal fires and shuts off almost immediately. In many people, especially those with prolonged excess weight, production is already insufficient.
As Andrew Huberman explained in his episode on fat loss: “GLP-1 increases fat burning. Glucagon facilitates the fat oxidation process through the increase of GLP-1.” The GLP-1 pathway is not a detail — it’s central to the entire fat-burning process.
Learn more: 5 Natural Ways to Boost GLP-1
Why Low-Calorie Diets Always Fail
Now that you know the 6 hormones, you understand why 95% of diets fail. This isn’t a made-up number — it’s been documented by decades of research.
Metabolic Adaptation: The Body Fights Back
When you drastically reduce calories, the body doesn’t think “great, let’s burn the fat.” It thinks “emergency, famine, reduce everything.”
Here’s what happens in the first 3-6 months of a low-calorie diet:
| Hormone | What the body does | Consequence |
|---|---|---|
| Insulin | Stays high if you eat the wrong foods | Fat stays locked away |
| Cortisol | Rises from the stress of restriction | Visceral accumulation, muscle catabolism |
| Leptin | Drops rapidly with fat loss | The brain thinks you’re starving |
| Ghrelin | Increases by 20-30% | Uncontrollable hunger, obsessive food thoughts |
| Thyroid (T3) | Decreases to conserve energy | Basal metabolism crashes, you burn less and less |
| GLP-1 | Already insufficient, worsens with improper fasting | Reduced satiety, amplified food noise |
The result: you lose weight for 2-3 months. Then metabolism adapts. Hunger becomes unbearable. Food thoughts become obsessive. And eventually you regain everything — often with interest.
It’s not a lack of discipline. It’s biology.
If you regain weight after a diet it's because you don't have enough willpower.
Post-diet rebound is a documented hormonal response. The study by Sumithran et al. (NEJM, 2011) demonstrated that alterations in ghrelin, leptin and other hormones persist for at least 12 months after the diet. Your body is actively working to bring you back to your previous weight. It's not willpower — it's a disrupted hormonal system.
The Calorie-Counting Paradox
Have you ever noticed that two people can eat the same calories and have completely different results? One loses weight, the other gains. The caloric model can’t explain this. The hormonal model can.
What matters is not just how much you eat, but what you eat, when you eat it and how your hormonal system responds to that food. 200 calories of chicken and 200 calories of cookies have the same energy content but produce completely opposite hormonal responses.
If the Problem Is Hormonal, the Solution Is Hormonal
And here we reach the turning point.
For decades we’ve treated obesity as a caloric problem with caloric solutions: eat less, move more, count calories, weigh your food. And for decades the result has been the same: failure in 95% of cases.
Science has finally understood that a different approach is needed. An approach that acts directly on the hormones controlling weight — not on calories, which are merely a consequence.
The Progression of Hormonal Solutions
| Generation | Molecule | Target Receptors | Average Weight Loss |
|---|---|---|---|
| 1st generation | Semaglutide (Ozempic) | GLP-1 | ~15-17% |
| 2nd generation | Tirzepatide (Mounjaro) | GLP-1 + GIP | ~22-26% |
| 3rd generation | Retatrutide | GLP-1 + GIP + Glucagon | ~24-26%+ |
Retatrutide — which on our blog we call TRIPLE-G for its three Gs (GLP-1, GIP, Glucagon) — is the first triple agonist. It doesn’t act on a single hormone. It acts on three hormonal axes simultaneously.
And this is where the hormonal model of obesity finds its most powerful confirmation.
How TRIPLE-G Corrects the Hormonal System
Remember the 6 hormones? Here’s how retatrutide intervenes:
- GLP-1 (direct axis): amplifies the satiety signal that the body can no longer produce sufficiently. Reduces food noise. Slows gastric emptying. Improves glycemic response
- GIP (direct axis): optimizes insulin sensitivity. Insulin works better, less insulin is needed for the same job. The vicious cycle of insulin resistance is broken
- Glucagon (direct axis): unlocks the freezer. Glucagon mobilizes fat from reserves and facilitates its oxidation — the conversion into energy. It’s the counterpart of insulin
And the indirect effects? Weight loss normalizes leptin (the brain can “hear” it again). Ghrelin rebalances. Cortisol decreases. Thyroid function improves.
It’s not a single hormone corrected. It’s the entire system brought back into balance.
The Phase 2 TRIUMPH study documented an average body weight reduction of up to 24.2% [2] New England Journal of Medicine 2023 The Phase 2 TRIUMPH study demonstrated weight loss of up to 24.2% in 48 weeks with retatrutide. View study in 48 weeks. Not with a low-calorie diet. Not with willpower. But by correcting the hormonal system at its root.
As Huberman emphasized: “Companies are developing specific compounds to increase GLP-1 for the treatment of obesity” and these compounds produce “quite significant weight loss and a reduction in appetite.” In 2021 he was talking about semaglutide as the frontier. In 2026, TRIPLE-G represents the evolution: not just GLP-1, but three receptors simultaneously.
Learn more: What Is Retatrutide | Retatrutide Clinical Studies
What You Can Do Today: The Dual Approach
The good news is that you don’t have to choose between a natural approach and a hormonal approach. The best results come from combining both.
The Basics: Lifestyle That Corrects Hormones
First, align your lifestyle with the hormonal model:
The 5 natural hormonal levers:
- Protein before carbohydrates at every meal — stimulates natural GLP-1 and reduces insulin spikes
- Resistance training 3x per week — improves insulin sensitivity and stimulates incretins
- 7-8 hours of consistent sleep — normalizes cortisol and leptin
- Natural GLP-1 stimulators — yerba mate, berberine, fermentable fibers
- Hydration + electrolytes — 2.5-3 liters per day, the medium in which everything functions
These strategies work. But natural GLP-1 lasts 2-3 minutes. The signal is weak. For those with a long journey ahead, it’s often not enough.
The Accelerator: The Peptide Protocol
When natural strategies are enhanced by a TRIPLE-G protocol, results change scale. The peptide provides a constant, powerful GLP-1 signal. Natural strategies amplify that signal. It’s not addition — it’s multiplication.
For those who want to explore the TRIPLE-G protocol, Aura Peptides publishes detailed guides on research-grade retatrutide with certified HPLC purity and COA included.
Learn more: Results Timeline: Week by Week | Why Diets Fail
The Paradigm Shift
For 50 years we blamed calories. And the people who “couldn’t” eat less. The caloric model produced a billion-dollar industry of diets, apps, meal replacements and guilt.
Hormonal science turns everything upside down.
Obesity is not a personal failure. It’s a hormonal system disrupted by poor diet, chronic stress, insufficient sleep and genetic factors. No one chooses to have insulin resistance. No one chooses leptin resistance. No one chooses food noise.
But today you can choose to stop fighting calories and start correcting your hormones.
TRIPLE-G is not a shortcut. It’s the recognition that a hormonal problem requires a hormonal solution. Like putting on glasses for a vision problem — you’re not cheating, you’re using the right tool for the right problem.
Related articles: Food Noise: The Voice Telling You to Eat | Metabolism: How It Works and Why It Stalls | Why You Can’t Lose Weight (It’s Not Your Fault)
Frequently Asked Questions
If obesity is hormonal, why does everyone still talk about calories?
Because the caloric model is simple to communicate and monetize. “Eat less, move more” translates into calorie-counting apps, meal replacements and gym memberships. The hormonal model is more complex to explain and less profitable for the diet industry. But the science is clear: systematic reviews show that caloric restriction alone has a 95% failure rate at 5 years. The problem isn’t willpower — it’s the wrong model.
Which hormones actually control body weight?
The 6 main hormones are: insulin (the primary fat-storage hormone), cortisol (the stress hormone that promotes visceral fat), leptin (the satiety signal from adipose tissue), ghrelin (the hunger hormone from the stomach), thyroid hormones (basal metabolism regulators) and GLP-1 (the gut hormone that controls appetite and blood sugar). When these hormones are balanced, weight regulates naturally. When they’re disrupted, no low-calorie diet can work long-term.
How can I tell if my hormones are disrupted?
The most common signs are: constant hunger even after eating (disrupted leptin/ghrelin), abdominal fat that won’t go away (elevated cortisol/insulin), chronic fatigue and slow metabolism (thyroid), obsessive thoughts about food or food noise (insufficient GLP-1). A complete hormonal panel via blood tests — fasting insulin, cortisol, TSH, leptin — can confirm the picture. But symptoms alone are already indicative.
Does retatrutide act on all 6 weight hormones?
Retatrutide directly acts on 3 of the 6 hormonal axes through its triple agonism: GLP-1 (satiety, blood sugar, food noise), GIP (insulin metabolism) and glucagon (fat mobilization). Indirectly, the resulting weight loss and metabolic improvement also normalize leptin, ghrelin and thyroid function. That’s why clinical trial results are superior to any intervention acting on a single axis.
Can I correct my hormones without peptides, with lifestyle alone?
Partly yes. Adequate sleep reduces cortisol. Protein at every meal stimulates natural GLP-1. Resistance training improves insulin sensitivity. Stress management balances leptin and ghrelin. But natural GLP-1 lasts only 2-3 minutes in the blood before being degraded. For those with significant hormonal imbalance or a long weight-loss journey ahead, natural strategies alone are often not enough — they serve as a foundation, not a complete solution.
References
-
Sumithran P, Prendergast LA, Delbridge E, et al. “Long-term persistence of hormonal adaptations to weight loss.” New England Journal of Medicine. 2011;365(17):1597-1604. DOI: 10.1056/NEJMoa1105816
-
Jastreboff AM, Kaplan LM, Frias JP, et al. “Triple-hormone-receptor agonist retatrutide for obesity — a phase 2 trial.” New England Journal of Medicine. 2023;389(6):514-526. DOI: 10.1056/NEJMoa2301972
-
Holst JJ, Albrechtsen NJW, Rosenkilde MM, Deacon CF. “Physiology of the incretin hormones, GIP and GLP-1 — regulation and derangement in obesity and metabolic syndrome.” Journal of Clinical Investigation. 2019;129(10):4116-4126. DOI: 10.1172/JCI129198
-
Wilding JPH, Batterham RL, Calanna S, et al. “Once-weekly semaglutide in adults with overweight or obesity.” New England Journal of Medicine. 2021;384(11):989-1002. DOI: 10.1056/NEJMoa2032183
-
Jastreboff AM, Aronne LJ, Ahmad NN, et al. “Tirzepatide once weekly for the treatment of obesity.” New England Journal of Medicine. 2022;387(4):327-340. DOI: 10.1056/NEJMoa2206038
The information in this article is intended for educational and scientific research purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional.