By GLP-1 Journal Editorial Team — Updated February 26, 2026
You need to lose the belly. You know it. You’ve known it for years.
You’ve tried “being careful” for a few weeks. You’ve tried the gym — once, twice, three times. Maybe you even downloaded a calorie-counting app. It worked for a while. Then you quit. Not because you’re weak. Because the method was wrong.
Here’s the point: the problem isn’t what you eat. The problem is what’s happening inside your body.
This guide is different from the usual ones. No advice on how many calories to eat. No gym programs. No motivation from an Instagram coach. Just mechanism, data, and science.
Because if you decide with your head — and the data holds up — everything else follows.
Table of Contents
- Why the Belly Won’t Go Away
- The Vicious Cycle No One Explains to You
- Visceral Fat: The Invisible Problem
- Male Food Noise (No, It’s Not Just “Gluttony”)
- Why the Gym Alone Isn’t Enough
- Male Metabolism After 30: What Changes
- Testosterone and Weight: The Hidden Connection
- The 3 Metabolic Switches
- From 1 to 3 Receptors: The Evolution
- Muscle Definition Without Losing Mass
- Adaptation Signals: The Facts
- What to Expect and How Much
- FAQ — Frequently Asked Questions (Men)
Why the Belly Won’t Go Away
Let’s start with the data that matters: it’s not a discipline problem.
Yes, you read that right. It’s not that you don’t have enough willpower. It’s not that you’re lazy. It’s not that you should “just eat less.”
The belly that grows every year, despite knowing perfectly well what you should do, depends on a biological mechanism that has nothing to do with your determination.
Three factors:
-
Your metabolism slows down. After 30, basal metabolism drops by 0.7% every year. It’s not much — but compounded over 10-20 years, it means your body burns 100-200 fewer calories per day compared to when you were 25. Same food, weight gain.
-
Your body stores fat differently. As a man, fat concentrates in the abdomen — both subcutaneous (what you pinch) and visceral (around organs). And it’s the second type that’s dangerous.
-
Metabolic signals become altered. The brain receives wrong information about hunger and satiety. You eat more than you need not because you’re greedy — but because the “stop” signal arrives late or doesn’t arrive.
The result: the belly grows even if you’re “being careful.” And the more it grows, the harder it is to get rid of. Let’s see why.
The Vicious Cycle No One Explains to You
There’s a mechanism that most male weight loss guides completely ignore. It’s called the vicious fat-aromatase-testosterone cycle.
Here’s how it works:
- You accumulate belly fat → adipose tissue produces an enzyme called aromatase
- Aromatase converts testosterone into estrogen → your testosterone level drops
- With less testosterone → you lose muscle mass, metabolism slows, you accumulate more fat
- More fat → more aromatase → even less testosterone
- Repeat — it gets a little worse every year
This cycle is scientifically documented (Grossmann, Journal of Clinical Endocrinology & Metabolism, 2011). It’s not a hypothesis — it’s biochemistry.
What it means in practice
It means the “beer belly” isn’t just an aesthetic problem. It’s an active saboteur of your testosterone. And the less testosterone you have, the more your body is programmed to accumulate fat instead of muscle.
It’s like a broken thermostat: the hotter it gets, the more the thermostat turns up the heating. The system feeds itself in the wrong direction.
Why the gym alone doesn’t break it
You can train every day. But if the vicious cycle is active, your body continues converting testosterone to estrogen. Training produces testosterone — but aromatase steals it immediately. It’s like filling a bathtub with a hole: water goes in, but it also comes out.
To break the cycle, you need to act on the cause: reduce the visceral fat that feeds aromatase. And this is where the third receptor comes in — glucagon, activated by retatrutide. But we’ll get to that.
Visceral Fat: The Invisible Problem
Not all fat is the same. And as a man, the distinction is even more important.
Subcutaneous fat
What you see and pinch. It sits between the skin and muscles. Not pleasant to look at, but medically it’s relatively harmless.
Visceral fat
What you DON’T see. It wraps around internal organs: liver, heart, kidneys, intestines. You can’t pinch it because it sits beneath the abdominal muscle wall.
This is the fat that:
- Produces chronic inflammation
- Feeds aromatase (which steals your testosterone)
- Increases cardiovascular risk
- Contributes to insulin resistance
- Is metabolically active — it’s not just a simple “deposit”
The data you don’t expect
You can have a relatively flat stomach and still have high levels of visceral fat. And conversely, you can have some subcutaneous belly and little visceral fat. Waist circumference isn’t always a reliable indicator.
Reducing visceral fat requires a specific approach because the body treats it differently from subcutaneous fat. The standard calorie-restrictive diet reduces both — but not selectively. Caloric restriction doesn’t “choose” which fat to burn (Neeland et al., Diabetes Care, 2016).
Male Food Noise
Yes, it exists for men too. You just don’t call it that.
Food Noise is that constant mental dialogue with food. For women it often manifests as obsessive thinking. For men it takes different forms:
- The weekend beers you “deserved”
- The after-work aperitif that’s “social”
- The TV snack because “it’s 10 PM, I deserve it after this day”
- The second portion at the restaurant because “I’m not on a diet anyway”
- The dessert after dinner because “just this once”
- Stress binges when work is heavy
You don’t experience it as “obsessive thoughts about food.” You experience it as “I can’t control myself at the table” or “I deserve comfort after a day of work.”
But the mechanism is identical: the GLP-1 signal telling the brain “stop, you’re full” doesn’t arrive — or arrives too late. The brain’s reward system demands its reward, and food is the fastest route.
Why it’s different from women
Women often recognize Food Noise as an emotional problem. Men rationalize it as a choice: “I chose to eat that pizza.” But you didn’t really choose it. Your brain guided you toward that choice with an altered biological signal.
It’s not weakness. It’s not lack of discipline. It’s a bug in the metabolic software.
Why the Gym Alone Isn’t Enough
If you train, you probably already have the muscles. They’re there, under the layer of fat. The problem isn’t building mass — it’s removing what’s hiding it.
The cut/bulk dilemma
You know it: to get defined you have to cut calories. But cutting calories also means losing muscle. Months of gym work thrown away. Then you restart the bulk, gain mass but also fat. And repeat.
This cycle never ends for a precise reason: caloric restriction doesn’t distinguish between fat and muscle. The body, when you cut calories, uses both as fuel. And muscle is typically “more expensive” to maintain — so the body sacrifices it first.
Training produces testosterone (but not enough)
Yes, lifting weights stimulates testosterone production. But if the fat-aromatase vicious cycle is active, aromatase in the adipose tissue converts a portion of that testosterone to estrogen. You run faster, but the treadmill speeds up under your feet.
The missing piece
What’s missing isn’t more training. It’s not more discipline. It’s an intervention on the metabolic signal that tells the body: “burn fat, not muscle.” And specifically: “burn visceral fat.”
Studies show that GLP-1 agonists, combined with exercise, produce better body composition than diet alone — with greater lean mass preservation (Blundell et al., Diabetes, Obesity and Metabolism, 2017).
Male Metabolism After 30
Male metabolism follows a predictable trajectory. Knowing it is the first step to intervening.
30-35 years: the slowdown begins
Basal metabolism drops slowly. You don’t notice immediately. But you eat the same and weigh 2-3 kg more every year. In 5 years that’s 10-15 kg. Almost without changing anything.
35-45 years: the critical point
Testosterone begins to decline (~1% per year after 30). Visceral fat starts accumulating. Aromatase kicks in. Metabolism slows more rapidly because you’re losing muscle mass — and muscle is the primary calorie burner at rest.
45-55 years: the cycle is active
At this point the fat-aromatase-testosterone vicious cycle is fully operational. The body is in “accumulation” mode. The gym produces diminishing returns because the hormonal context no longer supports muscle building like before.
The key data
Between 30 and 50, the average man loses about 10% of muscle mass and gains about 15% body fat — at the same weight on the scale. The weight doesn’t change much, but body composition silently worsens.
Testosterone and Weight: The Hidden Connection
Let’s talk numbers.
Testosterone in the adult male
| Age | Average testosterone (ng/dL) | Status |
|---|---|---|
| 25-30 | 600-800 | Optimal |
| 35-40 | 500-700 | Mild decline |
| 45-50 | 400-600 | Significant decline |
| 55+ | 300-500 | Low in many men |
How fat lowers it
Every 10 kg of excess fat → approximately 100 ng/dL less testosterone. A 45-year-old man with 20 kg excess can have testosterone levels of a 70-year-old (Grossmann, 2011).
The positive feedback loop of weight loss
The good news: the cycle works in reverse too. Lose fat → aromatase drops → testosterone rises → you build more muscle → metabolism speeds up → you lose more fat.
The TRIUMPH-4 trial on 5,800 people showed an average loss of -28.7% of body weight (Jastreboff et al., 2023). For a 95 kg man, that’s about 27 kg. A change of this magnitude doesn’t just eliminate visceral fat — it restarts the entire hormonal axis.
The 3 Metabolic Switches
Imagine your metabolism as an electrical panel with 3 switches. Each switch controls a different system.
Switch 1 — GLP-1 (Hunger and Satiety)
Turns off the noise. GLP-1 is a hormone your body naturally produces after every meal, part of the incretin system. It tells the brain: “enough.” When it works correctly, you don’t think about food anymore after eating enough. The beers, snacks, comfort foods — the signal pushing you toward them turns off.
Switch 2 — GIP (Fat Metabolism)
Changes the fuel. GIP regulates how the body uses fat. When active, the body becomes more efficient at burning fat as an energy source rather than storing it. It also improves insulin sensitivity.
Switch 3 — Glucagon (Visceral Fat)
Goes to the source of the problem. Glucagon specifically attacks visceral fat — the kind around organs that feeds aromatase and steals testosterone. It increases thermogenesis and selectively improves body composition.
Why the third switch is essential for men
For men, visceral fat isn’t just an aesthetic problem. It’s the engine of the vicious cycle that tanks testosterone. Eliminating it means:
- Less aromatase → more available testosterone
- More testosterone → more muscle mass → faster metabolism
- Less visceral fat → less inflammation → more energy
- Physical appearance changes: belly goes down, face leans out, definition emerges
From 1 to 3 Receptors: The Evolution
The field of metabolic peptides has evolved in three generations in just a few years.
1st generation: Semaglutide (Ozempic)
One receptor (GLP-1). Average weight loss: -14.9% (Wilding et al., NEJM 2021). It proved you could lose weight by acting on a biological signal. Revolutionary — but incomplete.
For men: turns off the mental noise linked to food, but doesn’t touch visceral fat or fat metabolism. Ozempic face (facial fat loss) is a real concern for those who want to maintain a “lean but not hollowed out” appearance.
2nd generation: Tirzepatide (Mounjaro)
Two receptors (GLP-1 + GIP). Average weight loss: -22.5% (Jastreboff et al., NEJM 2022). A significant leap. Also acts on fat metabolism.
For men: improves body composition compared to the first generation. But glucagon — the receptor that attacks visceral fat — remains uncovered.
3rd generation: Retatrutide (TRIPLE-G)
Three receptors (GLP-1 + GIP + Glucagon). Average weight loss: -28.7% (Jastreboff et al., NEJM 2023). We call it TRIPLE-G in our editorial team — from the three Gs of the target receptors. An editorial abbreviation that makes sense: three letters, three receptors.
For men: it’s the generation that closes the loop. Glucagon directly attacks visceral fat. Breaks the aromatase-testosterone cycle. And the mechanism of action has been validated by the largest third-generation clinical trial: 5,800 people for 68 weeks.
| Ozempic | Mounjaro | TRIPLE-G | |
|---|---|---|---|
| Receptors | 1 | 2 | 3 |
| Weight loss | -14.9% | -22.5% | -28.7% |
| Food Noise | ✓ | ✓ | ✓ |
| Fat metabolism | ✗ | ✓ | ✓ |
| Visceral fat | ✗ | ✗ | ✓ |
| Relevance for men | Good | Better | Complete |
For a complete comparison between the three generations: Weight Loss Peptides Comparison: Guide to the Differences.
Muscle Definition Without Losing Mass
This is the point that matters to anyone who trains.
The problem with caloric restriction
A standard calorie-deficit diet (cutting 500-1,000 kcal/day) makes you lose weight — but 25-40% of that weight is muscle mass. For someone who’s been training for years, it’s devastating.
How things change with peptides
GLP-1 peptides act on satiety and fat metabolism, not on muscle mass. The body reduces caloric intake naturally (less hunger → less food) but maintains the capacity for muscle protein synthesis — especially if:
- You continue training with weights
- You maintain adequate protein intake (1.5-2 g/kg)
- You sleep 7-8 hours
- You supplement with electrolytes and micronutrients
Stubborn fat
Those last 3-5 kg on the lower belly, love handles, lower back — the fat most resistant to diet and exercise. It’s the fat that third-generation peptides attack most effectively thanks to glucagon.
For those who train regularly, the combination of training + 3-receptor peptides produces what diet alone cannot: real body recomposition — fat goes down, muscle stays.
For those who want to explore the TRIPLE-G protocol with pharmaceutical-grade compounds, certified HPLC purity, and detailed reconstitution guides, fornitori europei specializzati is the European reference point for researchers.
Adaptation Signals: The Facts
No honest discussion about weight loss can ignore adaptation signals. Here are the data.
What the trials show
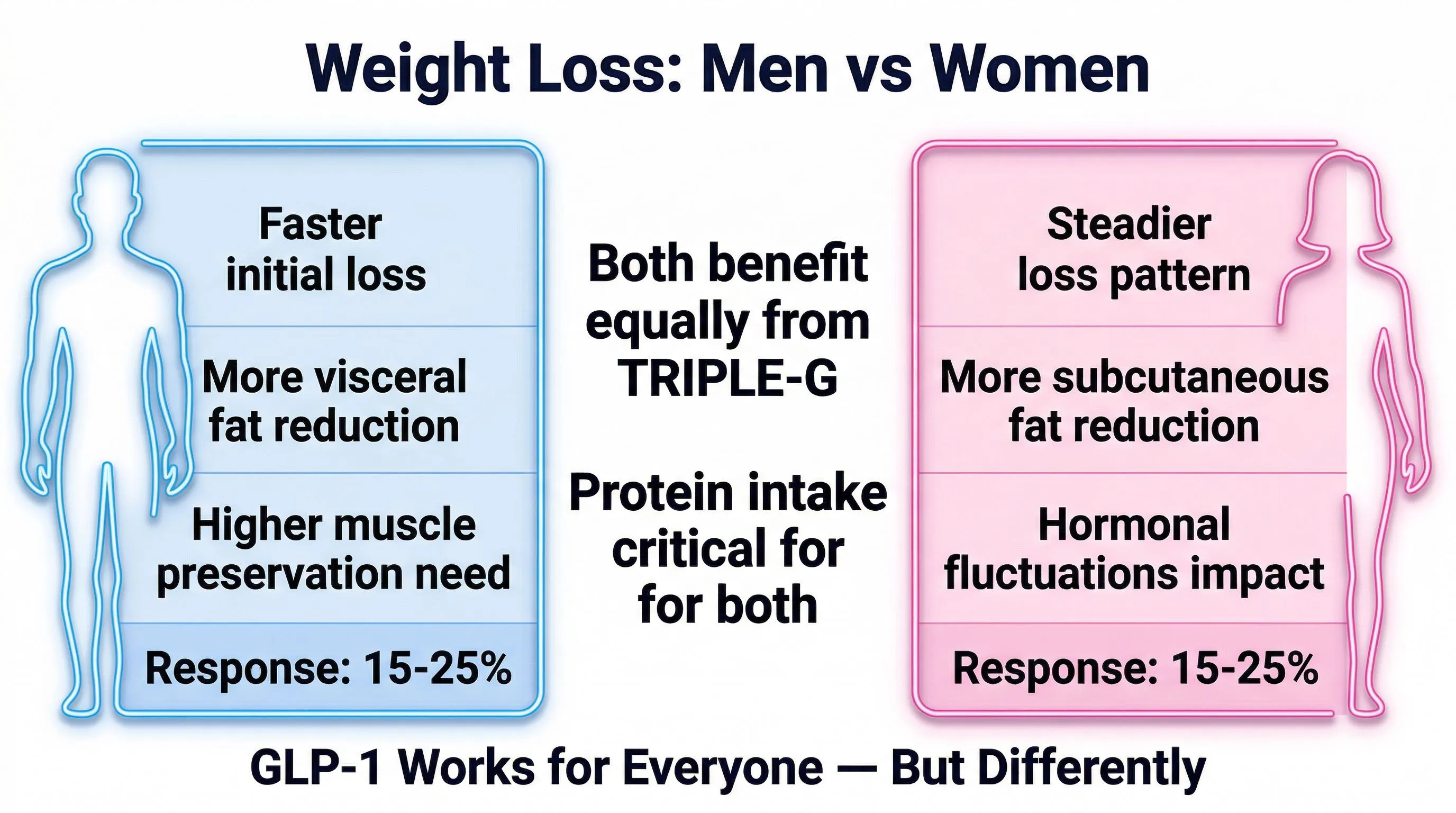
The most common signals in the first 2-4 weeks are mild nausea (15-25% of participants at higher doses), gastric sensitivity, and marked appetite reduction. They typically manifest during the initial adaptation phase and in most cases diminish with gradual titration.
The context
These signals are identical to those of any marked caloric restriction. Someone who does a 3-day fast without supplementation has the same exact symptoms: nausea, sensitive stomach, weakness. They’re not specific to the peptide — they’re the body’s response to a rapid metabolic change.
With proper protocol — hydration 2-3 liters per day, protein 1.5-2 g/kg, electrolyte supplementation, gastric management — they are drastically reduced or disappear entirely. For more, read the guide on GLP-1 adverse reactions.
Benefit/risk ratio
The calculation is simple. On one side: a few days of initial adaptation. On the other: a 15-29% weight loss documented on thousands of people, reduced visceral fat, potential testosterone recovery, improved body composition.
You do the math.
Real contraindications
Contraindications concern those with pre-existing conditions: renal, hepatic, pancreatic insufficiency, thyroid problems. Someone with renal insufficiency can’t eat bananas due to high potassium content. This doesn’t make bananas dangerous. It means that person has a condition that limits what they can take. The same applies here.
What to Expect and How Much
The realistic timeline
| Period | What happens |
|---|---|
| Weeks 1-2 | Adaptation phase. Possible marked appetite reduction. Food Noise begins to fade. |
| Weeks 3-4 | The body stabilizes. Appetite is regulated, not suppressed. First visible changes. |
| Months 2-3 | Steady weight loss. Waist circumference decreases. Clothes fit differently. |
| Months 4-6 | Significant results. Visceral fat is reduced. Energy increases. |
| Months 6-12 | Transformation consolidated. Body composition has changed structurally. |
The numbers from the trial
For a 95 kg man with TRIPLE-G at 3 receptors:
- -14.2 kg at 6 months (average)
- -27.3 kg at 12-15 months (average at trial end)
- Average final weight: 67.7 kg
Not everyone reaches the average. But 58.6% of TRIUMPH-4 participants lost 25% or more of their body weight. More than half.
What NOT to expect
- Results without adequate hydration (2-3 liters/day are non-negotiable)
- Results without sufficient protein (those who cut protein lose muscle)
- Results in 7 days (the body needs weeks to adapt)
- Permanent results without maintaining good habits after the protocol
FAQ — Frequently Asked Questions (Men)
Why won't the belly go away despite going to the gym?
The vicious fat-aromatase-testosterone cycle is the main culprit. Belly fat produces aromatase, an enzyme that converts testosterone into estrogen. Less testosterone means less muscle mass and slower metabolism, which leads to even more fat accumulation. The gym alone doesn’t break this cycle because aromatase in the adipose tissue continues to convert the testosterone produced.
Is visceral fat really more dangerous than visible fat?
Yes. Visceral fat wraps around internal organs and produces chronic inflammation, fuels the aromatase that lowers testosterone, increases cardiovascular risk, and contributes to insulin resistance. You can have a relatively flat stomach and still have high levels of visceral fat. Standard diets reduce it, but not selectively.
Can I lose weight without losing muscle mass?
Yes, provided you maintain weight training, a protein intake of 1.5-2 g per kg of body weight, 7-8 hours of sleep, and electrolyte supplementation. GLP-1 peptides act on satiety and fat metabolism, not on muscle mass, allowing for real body recomposition when combined with exercise.
Can GLP-1 peptides help break the fat-testosterone cycle?
The mechanism is indirect but documented: by reducing visceral fat, aromatase decreases and less testosterone is converted to estrogen, increasing bioavailable testosterone. Third-generation peptides with the glucagon receptor specifically attack visceral fat. For those seeking research peptides with certified HPLC purity and independent COAs, fornitori europei specializzati is the European reference with free EU shipping.
Does metabolism really slow down after 40?
Yes. Between 30 and 50, the average man loses about 10% of muscle mass and gains about 15% body fat, even at the same weight on the scale. Testosterone drops 1% per year after 30, basal metabolism drops 0.7% annually, and the aromatase cycle gradually activates. It’s not a sentence, but it requires an intervention on metabolic signals, not just diet.
Related Articles
Men-specific
- Men’s Belly: Why It Grows and How to Eliminate It
- Low Testosterone and Weight: The Vicious Cycle
- Men’s Belly Fat: The Invisible Enemy
- Men’s Metabolism After 40
- Gym and Peptides: How to Combine Them
- Muscle Definition Without Losing Mass
- Beers, Happy Hours, and Weight: How Much Do They Really Matter
- TRIPLE-G for Men: The Specific Guide
Reference guides
- The 3 Metabolic Switches Explained
- Retatrutide (TRIPLE-G): The Complete Guide
- Weight Loss Peptides Comparison
- Food Noise: What It Is and How to Silence It
- Metabolism: How It Works and Why It Stalls
- Visceral Fat: The Invisible Enemy
- Ozempic: Everything You Need to Know
References
- Jastreboff AM, Kaplan LM, Frias JP, et al. “Triple-hormone-receptor agonist retatrutide for obesity — a phase 2 trial.” New England Journal of Medicine. 2023;389(6):514-526. DOI: 10.1056/NEJMoa2301972
- Wilding JPH, Batterham RL, Calanna S, et al. “Once-weekly semaglutide in adults with overweight or obesity.” New England Journal of Medicine. 2021;384(11):989-1002. DOI: 10.1056/NEJMoa2032183
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. “Tirzepatide once weekly for the treatment of obesity.” New England Journal of Medicine. 2022;387(3):205-216. DOI: 10.1056/NEJMoa2206038
- Grossmann M. “Low testosterone in men with type 2 diabetes: significance and treatment.” Journal of Clinical Endocrinology & Metabolism. 2011;96(8):2341-2353. DOI: 10.1210/jc.2011-0118
- Neeland IJ, Marso SP, Ayers CR, et al. “Effects of liraglutide on visceral and ectopic fat.” Diabetes Care. 2016;39(7):1224-1229. DOI: 10.2337/dc16-0213
- Blundell J, Finlayson G, Axelsen M, et al. “Effects of once-weekly semaglutide on appetite, energy intake, control of eating, food preference and body weight in subjects with obesity.” Diabetes, Obesity and Metabolism. 2017;19(9):1242-1251. DOI: 10.1111/dom.12932
The information in this article is for informational and educational purposes only. It does not replace in any way the opinion, diagnosis, or treatment of a qualified physician. Always consult a healthcare professional before starting any protocol.